Moving and Positioning Clients
Key Points
- Immobile residents require routine repositioning to prevent pressure injuries and immobility complications.
- Lift sheets reduce friction and shear and should be used for assisted bed movement.
- Correct alignment, pressure-relieving supports, and position rotation schedules improve safety and comfort.
- Position selection should match clinical purpose (for example Fowler’s for meals/oral care and aspiration reduction, Sims’ for rectal procedures, prone/tripod for selected respiratory support, and Trendelenburg in limited emergency indications).
- Post-surgical or prolonged-bedrest positioning plans should actively prevent hip malalignment and foot-drop complications.
- Intraoperative positioning must balance operative exposure with pressure, nerve, and circulatory protection through team-based monitoring.
Pathophysiology
Immobility concentrates pressure over bony prominences and impairs local perfusion, increasing risk of tissue ischemia and pressure injury. Repeated friction and shear further damage fragile skin and subcutaneous tissue.
Older adults are highly susceptible because skin integrity and cushioning decline with age. Poor repositioning technique can create skin tears, bruising, and musculoskeletal strain in both resident and caregiver.
Therapeutic positioning also affects respiratory expansion, aspiration risk, and circulation. Position choice therefore links directly to comfort, oxygenation, and skin outcomes.
Classification
- Repositioning frequency: Routine at least every two hours, with hourly schedules for higher-risk skin cases.
- Pressure-relief tools: Lift sheets, pillows, wedges, foam boots, and foot cradles.
- Pressure-relief surfaces: Specialty mattresses/overlays (foam, gel, low-air-loss, alternating-pressure) selected by risk and tissue status.
- Alignment-support tools: Abductor pillows and foot-positioning orthotics (for example podus boot) that maintain near-neutral joint alignment.
- Core positions: Supine, prone, lateral, Sims’, Fowler’s/high Fowler’s, semi-Fowler’s, Trendelenburg/reverse Trendelenburg, lithotomy, and tripod.
- Position-definition cues: Tripod (orthopneic) is seated forward-leaning support (often onto an overbed table); prone is abdomen-down; lateral is side-lying with top leg flexed for support; Sims’ is semiprone between prone and lateral.
 Illustration reference: OpenStax Clinical Nursing Skills Ch.9.
Illustration reference: OpenStax Clinical Nursing Skills Ch.9.
 Illustration reference: OpenStax Clinical Nursing Skills Ch.9.
Illustration reference: OpenStax Clinical Nursing Skills Ch.9. - Technique focus: Slide with lift sheet rather than lifting/pulling directly on limbs or skin.
- Position-specific use: Fowler’s for eating/drinking, oral care, aspiration reduction, and oxygenation support; semi-Fowler’s for similar goals with lower coccyx pressure over longer periods; Sims’ for enema/suppository preparation and semiprone procedural setup; lateral for coccyx offloading and selected pregnancy positioning (and selected operative hip/kidney/thoracic access); prone/tripod for selected respiratory support (and selected intraspinal procedural setup); lithotomy for gynecologic/urologic access; Trendelenburg variants for selected emergency or pelvic/abdominal visualization contexts per orders/protocol.
Nursing Assessment
NCLEX Focus
Priority questions often ask which positioning choice best protects skin while supporting breathing and safety.
- Assess skin over bony prominences for redness, tenderness, or early breakdown.
- Prioritize high-risk pressure points (coccyx, heels, ears, and device-contact areas such as nasal tubing sites) because injury can develop within hours in bedbound patients.
- Verify pressure-injury risk screening is current (for example Braden at shift start and with condition changes) and align turning schedule to current risk level.
- Verify spinal alignment and centered bed position after each turn.
- In perioperative or prolonged-procedure contexts, assess neurovascular status and hemodynamic tolerance after position changes.
- In high-risk positioning contexts, assess for early compartment-syndrome and peripheral-nerve-palsy cues (new swelling, escalating pain, numbness, weakness, reduced perfusion).
- Identify friction/shear risk patterns, especially in Fowler’s when sliding downward.
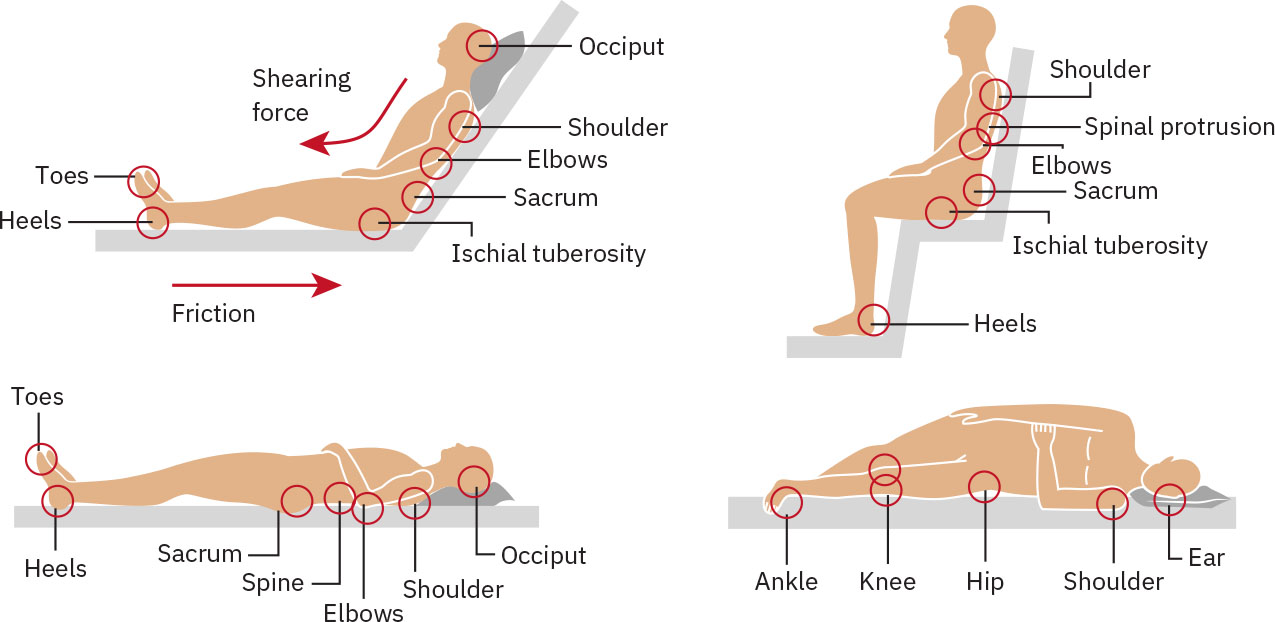 Illustration reference: OpenStax Clinical Nursing Skills Ch.9.
Illustration reference: OpenStax Clinical Nursing Skills Ch.9. - Monitor repositioning adherence and document move-from/move-to position with time.
Nursing Interventions
- Use a lift sheet for assisted repositioning to reduce friction and shear.
- Coordinate two-person boosts with count-based movement and neutral body mechanics.
- For “move up in bed” boosts, place a protective pillow at headboard, fan-fold draw sheet for secure grip, cue chin tuck/arms crossed/knees bent, and slide (do not lift) on coordinated count.
- Float heels using pillow under calves or use ordered pressure-relief devices.
- Rotate among supine and side-lying positions per care plan to offload pressure points.
- In operative settings, coordinate position setup collaboratively so procedural access is preserved while pressure points and nerve pathways are protected.
- In prolonged or high-risk positioning, protect eyes and airway alignment and verify secure transfer setup to reduce eye injury, airway compromise, and fall events.
- Use passive or assisted repositioning based on patient capability, with pillows/wedges or other aides to offload vulnerable tissue.
- Reposition at least every two hours unless higher-frequency plans are indicated, and complete focused skin checks with each position change.
- For post-hip-surgery restrictions, maintain neutral hip alignment with ordered abductor support and avoid prohibited hip motions during bed and seated positioning.
- For foot-drop prevention in prolonged supine bedrest, maintain ankle positioning near 90 degrees with ordered orthotic support.
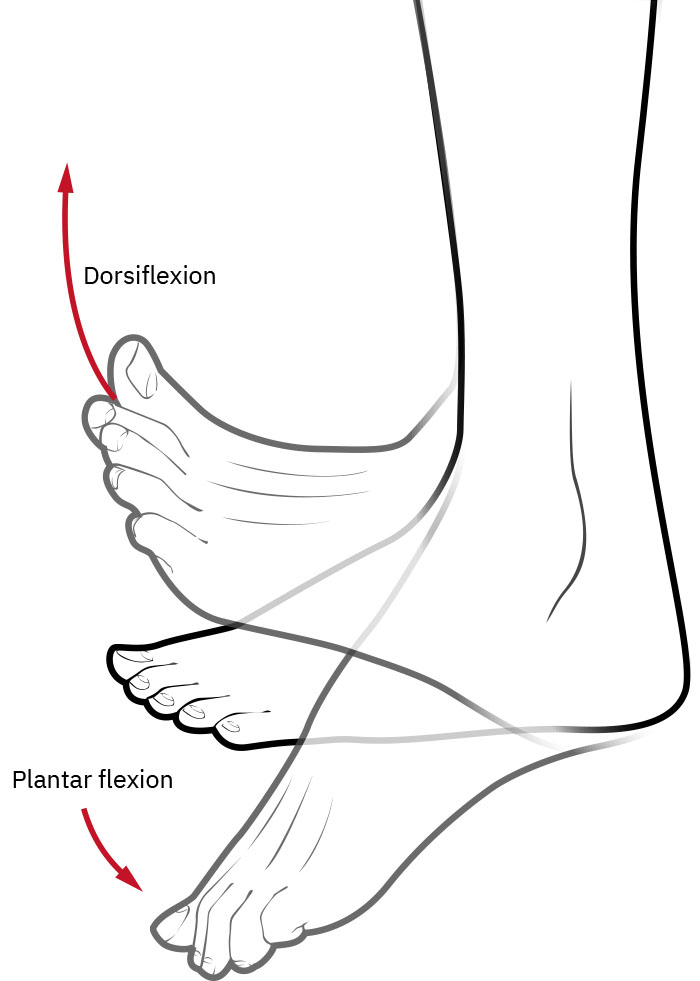 Illustration reference: OpenStax Clinical Nursing Skills Ch.9.
Illustration reference: OpenStax Clinical Nursing Skills Ch.9. - Inspect and reposition medical-device contact points (for example oxygen tubing at nares/ears) to reduce device-related pressure injury.
- Ensure lines/tubes/devices are never trapped under the patient after turns or boosts.
- Use adaptive supports for alignment and skin protection (for example wedges behind back, heel protectors, rolled towels/washcloths for hand contracture positioning and moisture control).
- For bed-bound clients, keep head-of-bed elevation around 30-45 degrees when not contraindicated to support lung expansion.
- In prone positioning, place supports to maintain leg/foot alignment and monitor oxygenation response in clients with respiratory compromise.
 Illustration reference: OpenStax Clinical Nursing Skills Ch.9.
Illustration reference: OpenStax Clinical Nursing Skills Ch.9. - In Fowler’s positioning, reduce sliding-related shear by raising the lower bed section or supporting lower legs with pillows to bend the knees.
- For residents with existing pressure injuries or highly susceptible areas, follow hourly repositioning schedules and document move-from/move-to position and time.
- Keep bed low/locked and call light reachable after each repositioning event.
Shear and Skin Injury Risk
Pulling residents on linens without a lift sheet or allowing prolonged unrelieved pressure can cause preventable skin damage and is unsafe care.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| analgesics | Pre-turn pain-management contexts | Coordinate repositioning after pain control to improve participation and reduce guarding. |
| sedatives | Rest-promoting medications | Sedation can reduce spontaneous movement; reinforce scheduled repositioning vigilance. |
Clinical Judgment Application
Clinical Scenario
A bedbound resident with heel redness and coccyx discomfort slides downward repeatedly in Fowler’s position.
- Recognize Cues: Pressure risk at heels/coccyx with visible shear pattern.
- Analyze Cues: Current positioning strategy is causing recurrent friction and pressure loading.
- Prioritize Hypotheses: Highest priority is immediate pressure offloading and shear reduction.
- Generate Solutions: Use lift sheet for boost, float heels, adjust lower bed section, and rotate to lateral offloading schedule.
- Take Action: Implement repositioning plan and report skin changes to nurse.
- Evaluate Outcomes: Pressure sites improve and resident comfort increases without new skin injury.
Related Concepts
- body-mechanics-and-safe-equipment-use - Caregiver mechanics influence repositioning safety and injury prevention.
- immobility-complications - Regular repositioning reduces pulmonary, circulatory, and skin complications.
- making-an-occupied-bed - Linen and turning workflows intersect during in-bed care.
- fall-prevention - Post-reposition bed safety checks prevent accidental injury.
- documenting-and-reporting-data - Time-position documentation supports skin-risk tracking.
Self-Check
- Why is lift-sheet sliding safer than direct pulling on skin or limbs?
- Which position-related factor increases shear risk in Fowler’s position?
- What should be documented after each repositioning event for high-risk residents?