Integumentary System
Key Points
- The integumentary system protects against injury, infection, and fluid loss.
- Core structures include skin, hair, and nails with layered barrier and sensory functions.
- The integumentary system is the body’s largest organ-level system.
- Skin findings can signal dysfunction in other body systems (for example cyanosis with inadequate perfusion).
- Skin-integrity impairment can involve superficial skin layers or deeper tissues, with different escalation needs.
- Aging skin is thinner and more fragile, increasing risk for tears and pressure injuries.
- CNA prevention priorities include moisture control, pressure relief, and friction/shear reduction.
Pathophysiology
The integumentary system includes skin and associated structures that form a protective barrier. The three major skin layers are the epidermis (outer protective surface), dermis (vascular and sensory support layer containing follicles and glands), and hypodermis or subcutaneous layer (adipose-rich cushioning and insulation).
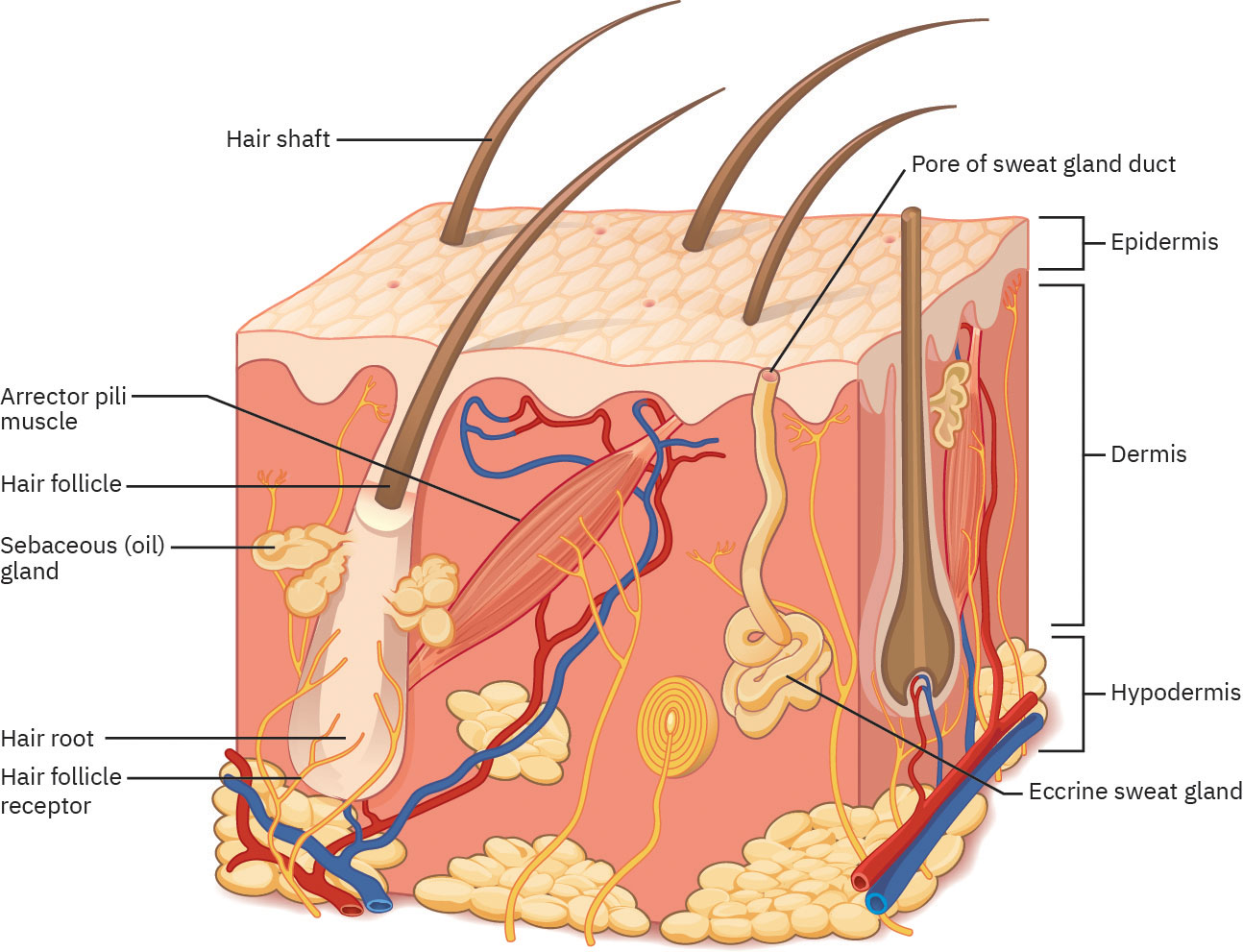 Illustration reference: OpenStax Clinical Nursing Skills Ch.21.1.
Illustration reference: OpenStax Clinical Nursing Skills Ch.21.1.
The epidermis is a thin epithelial barrier that protects deeper tissues from water loss, mechanical and chemical trauma, microorganism exposure, and ultraviolet injury. Most body sites have four epidermal strata, while palms and soles have five (including stratum lucidum). Deep-to-superficial epidermal strata are stratum basale, spinosum, granulosum, lucidum (thick skin), and corneum. Melanocytes in the basale produce melanin that helps protect keratinocytes and superficial nerve endings from ultraviolet injury and contributes to skin color. Keratinocytes produce keratin, a water-repellent structural protein that strengthens barrier function. Skin color expression is shaped by melanin, carotene, and hemoglobin, and localized melanocyte clustering can present as freckles. After new ultraviolet exposure, melanin synthesis rises over several days and commonly peaks at about 10 days, so early sun exposure can still produce sunburn before maximal pigment protection develops. Merkel cells in the basale support light-touch sensation, and Langerhans cells in the spinosum support first-line immune surveillance; physiology framing also identifies a bone-marrow origin pathway for these antigen-presenting cells. In the granulosum, glycolipid-rich barrier formation and keratinization reduce transepidermal water loss. The stratum corneum is the thickest epidermal layer (about three quarters of epidermal thickness) and contributes antimicrobial host defense through barrier peptides.
The epidermis includes sweat-duct openings and the visible hair shaft. The dermis contains hair follicles, sebaceous glands, blood vessels, sweat glands, and nerve endings. Beneath the hypodermis are deeper structures such as muscle, ligaments, and tendons. Integumentary glands are exocrine structures that release secretions through ducts onto epithelial surfaces, unlike endocrine glands that release hormones directly into the bloodstream. The dermis has a superficial papillary layer and deeper reticular layer. Together they provide vascular support, pain-touch sensing, thermoregulation, structural collagen support, and nutrient delivery to the epidermis. Sebaceous glands are present in most skin (except palms and soles) and secrete sebum that helps waterproof skin and hair. Eccrine glands are broadly distributed and support heat loss by sweat evaporation, while apocrine glands (axilla, perineum, areola) become more active after puberty and may secrete a milky sweat. Eccrine sweat is hypotonic and includes water, sodium chloride, trace metabolic waste, antibodies, and antimicrobial peptides (for example dermcidin), which adds barrier-defense value beyond cooling alone. Apocrine secretions contain thicker organic components that are more prone to bacterial decomposition and odor. The hypodermis anchors skin to underlying tissue, cushions against trauma, stores major fat reserves (about half of the body’s adipose cells), and supports vascular-lymphatic transport. Skin function also has psychosocial impact because visible skin appearance influences self-image and social interaction. Arrector pili muscle contraction produces piloerection (goosebumps) as part of sympathetic fight-or-flight response and limited heat-conservation effort.
Hair is formed from keratinized cells. The hair root inside the follicle is the living portion, while the shaft above skin is nonliving. Hair follicles are distributed across most body surfaces except mucous membranes, lips, palms, and soles. Perifollicular hair-root plexus innervation makes hair highly sensitive to light environmental movement and contact.
Nails are hard keratinized structures that support fingertip protection, sensation, and fine-task function. Basic anatomy includes root, plate, and free margin with supporting nail bed and surrounding folds.
With aging and chronic illness, dermal thickness and elasticity decline, reducing tolerance to pressure, moisture, and friction. Reduced oil and sweat production increase dry-skin cracking and pruritus risk and weaken thermoregulation, raising heat-illness vulnerability. Melanin-pattern changes may produce uneven pigmentation with focal hyperpigmented or hypopigmented areas. Elastic-fiber degeneration and adipose redistribution can increase wrinkling and sagging, and reduced skin recoil may appear as tenting that can also signal dehydration when persistent. Age-related decline in epidermal mitotic activity slows wound healing and contributes to reduced pressure/pain sensation, and older-adult wound healing may be up to about four times slower than in younger adults.
In infants and young children, thermoregulation and barrier maturity are incomplete. Infant skin is thinner, less pigmented, and more loosely attached at the epidermal-dermal interface, with lower subcutaneous insulation and higher permeability; this increases heat loss, friction injury/blister risk, UV vulnerability, and absorption of topical substances. In preterm newborns, the dermal-epidermal junction is weaker and includes lower collagen, water, and melanin reserve, increasing fragility and infection risk. Sebaceous glands are present in children but remain relatively inactive until puberty.
Sustained pressure over bony prominences impairs perfusion and can cause localized tissue injury. Shear and friction accelerate epidermal separation and skin tears.
Skin absorption has direct medication and toxin implications: transdermal therapies can deliver local/systemic effects (for example scopolamine, estrogen/testosterone, nicotine, selected opioids/contraceptives), and accidental contact exposure can occur without barrier protection. For high-risk transdermal drugs (for example fentanyl), use gloves and contact precautions because unintended dermal absorption can cause harm. Skin elimination through perspiration removes water, electrolytes, and small nitrogenous wastes (for example urea, uric acid, ammonia) while supporting thermal balance. Skin-initiated vitamin D synthesis begins with UV conversion of 7-dehydrocholesterol to cholecalciferol, followed by liver and kidney hydroxylation to active calcitriol. Population-level variation exists in sweat-gland activity, body-odor patterns, melanin distribution, and heat acclimatization response.
Because skin injury increases infection and immobility risk, prevention-focused daily care is essential.
Classification
- Barrier function: Protection from pathogens, trauma, and fluid imbalance.
- Physiologic-function domain: Protection, thermoregulation, sensation, absorption/elimination, and vitamin D synthesis support.
- Layered anatomy: Epidermis, dermis, and hypodermis each support distinct protection, sensation, and cushioning roles.
- Accessory structures: Hair and nails contribute to insulation, sensation, protection, and functional support.
- Integrity-diagnosis axis: impaired-skin-and-tissue-integrity differentiates superficial skin-layer injury from deeper tissue injury.
- Pressure-related risk: Tissue injury from prolonged compression and shear.
- Moisture-associated risk: Maceration from incontinence or perspiration.
- Aging vulnerability: Thin, fragile skin with reduced healing reserve.
Nursing Assessment
NCLEX Focus
Priorities include early recognition of non-blanchable redness and prevention strategies for high-risk residents.
- Inspect bony prominences and skin folds for redness, breakdown, moisture damage, or tears.
- In inpatient workflows, complete and document baseline comprehensive skin assessment within about 24 hours of admission, then continue serial reassessment per status/policy.
- Include high-risk inspection zones: bony prominences, skin folds/perineum, spaces between fingers/toes, and skin under removable medical devices.
- Distinguish perfusion-pattern findings that increase tissue-injury risk:
- arterial pattern: cool/pale skin, exertional pain, ischemic-ulcer trend
- venous pattern: edema, brown leathery lower-leg skin, weeping-ulcer trend
- Adapt skin-color assessment to baseline pigmentation; in darker skin, evaluate mucous membranes (for example gums/palpebral conjunctiva) when screening for pallor.
- For jaundice screening across skin tones, inspect sclera and hard palate in addition to general skin color; report new-onset jaundice promptly.
- Recognize pigmentation-pattern differences across skin tones; darker skin may show postinflammatory hyperpigmentation, keloid tendency, and other nonmalignant pigment changes.
- In darker skin, include pattern recognition for dermatosis papulosa nigra, vitiligo, pityriasis-type scaling, and dry-skin/hair-loss presentations when differentiating normal variation from pathology.
- Assess mobility limits that increase pressure duration.
- Identify friction/shear sources during repositioning and transfers.
- Assess sensation deficits (for example diabetic neuropathy) and reinforce daily foot inspection for unrecognized trauma.
- In newborns and infants, screen for both heat loss and overheating; thermal dysregulation can present as flushed/warm skin, heat rash, damp hair/sweating, tachycardia, tachypnea, fussiness, lethargy, or unresponsiveness.
- In infants, expect benign neonatal skin variants (for example transient acne-like eruptions and relatively rough early neonatal texture) while still escalating progressive inflammatory/infectious changes.
- Use infant thermal-safety counseling: avoid over-bundling/heating pads, support ventilation, and target room temperature near 68 to 72 degrees F (20 to 22 degrees C).
- In pediatric and adolescent groups, screen for activity-related skin injury risk and common school-age infectious skin problems (for example head lice, impetigo, scabies, tinea-infection, varicella) while preserving age-appropriate autonomy in teaching.
- In prepubescent and adolescent stages, reassess sebum-production changes because rising sebaceous activity increases acne-prone patterns.
- If diffuse rash-like red spots are present, perform blanching assessment; nonblanching petechiae or purpura require urgent provider notification.
- Include capillary-refill assessment at nail beds when perfusion concern exists; brisk return is expected (commonly within about 2 seconds), while persistent delay (for example >3 seconds) warrants escalation context review.
- Use skin turgor cautiously for dehydration screening, especially in older adults where age-related elasticity loss reduces reliability.
- If edema is present, distinguish pitting from nonpitting and grade pitting severity by depth and rebound time (1+ to 4+) to trend progression.
- For unilateral limb swelling with known or suspected lymphedema, protect the limb from avoidable constriction/trauma and follow limb-alert restrictions (for example avoid blood-pressure cuffs on the affected extremity when ordered).
- Treat unusual bruise or burn distribution patterns as potential abuse/neglect indicators requiring policy-based escalation and reporting.
- Differentiate dermal melanocytosis from bruising in infants: congenital blue-gray patches are typically nonblanchable and commonly fade over time.
- For patients with cognitive impairment, simplify skin-check coaching, involve caregivers, and use developmentally appropriate communication during assessment.
- Match communication style and exam steps to developmental level (for example caregiver-lap infant exam versus direct school-age/adolescent engagement) to improve assessment reliability and participation.
- Report early skin changes promptly to nurse for timely intervention.
Nursing Interventions
- Reposition dependent residents on schedule and offload pressure points.
- Keep skin clean, dry, and protected after incontinence episodes.
- Support hydration/nutrition and regular moisturizing of dry skin while keeping skin folds clean and fully dry.
- In immediate newborn care, reduce heat loss with thorough drying after birth/bathing, prewarmed blankets/caps, draft avoidance, and skin-to-skin support when stable.
- For infants and dependent children, teach caregivers protective routines (trimmed nails or mittens, lukewarm bathing, and prompt rash/lesion reporting).
- Reinforce infant skin-absorption precautions (for example avoid nonessential topical products in young infants and use age-appropriate guidance for sun/skin products).
- Use lift-sheet techniques instead of dragging to reduce shear.
- Smooth linens and avoid wrinkles under pressure areas.
- Implement ordered pressure-relief surfaces and support devices.
Avoidable Injury Risk
Missed repositioning, unmanaged moisture, or rough handling can lead to preventable skin breakdown and complications.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| topical-skin-protectants | Barrier creams | Apply per care plan to reduce moisture-associated damage risk. |
| antibiotics | Skin-infection treatment contexts | Early skin-change reporting supports timely treatment escalation. |
Clinical Judgment Application
Clinical Scenario
A bedbound resident with incontinence develops persistent heel redness and sacral moisture irritation.
- Recognize Cues: Pressure and moisture injury precursors.
- Analyze Cues: Current prevention plan is insufficient for risk level.
- Prioritize Hypotheses: Immediate priority is pressure offloading and moisture control.
- Generate Solutions: Increase repositioning reliability, float heels, apply barrier care, and improve linen smoothness.
- Take Action: Implement interventions and report findings to nurse.
- Evaluate Outcomes: Skin integrity stabilizes without progression to open injury.
Related Concepts
- moving-and-positioning-clients - Repositioning technique directly affects shear and pressure risk.
- impaired-skin-and-tissue-integrity - Provides NANDA-aligned depth distinction and high-risk wound-healing factors.
- immobility-complications - Immobility increases skin breakdown vulnerability.
- making-an-occupied-bed - Linen management influences moisture and friction exposure.
- body-mechanics-and-safe-equipment-use - Safe handling reduces skin trauma during movement.
- documenting-and-reporting-data - Objective skin-change documentation supports timely care escalation.
- tinea-infection - Common pediatric and adolescent fungal skin-pattern recognition and prevention.
- varicella - Contagious pediatric vesicular rash pattern with isolation and complication-screening priorities.
Self-Check
- Which daily care actions most reduce pressure-injury risk?
- Why does shear cause deeper tissue damage even when skin appears intact early on?
- What findings should be reported immediately for skin-integrity escalation?