Rheumatoid Arthritis Autoimmune Joint Disease
Key Points
- Rheumatoid arthritis (RA) is a chronic systemic autoimmune disorder targeting synovial tissue.
- Population burden is substantial (about 1% globally; about 1.3 million U.S. adults in estimates) and RA remains a major work-disability contributor.
- Typical presentation is bilateral, symmetrical inflammatory joint pain, swelling, and prolonged morning stiffness.
- RA often follows a remission-exacerbation pattern with intermittent symptom flares.
- During pregnancy, symptoms may improve for some patients, but risk can remain elevated for cesarean delivery, preeclampsia, and preterm birth.
- Disease progression can cause deformity, contractures, and functional decline without early treatment.
- Core treatment combines symptom control with disease-modifying therapy to slow joint damage.
- Nursing priorities focus on pain control, mobility preservation, skin/joint protection, and infection-risk teaching.
Pathophysiology
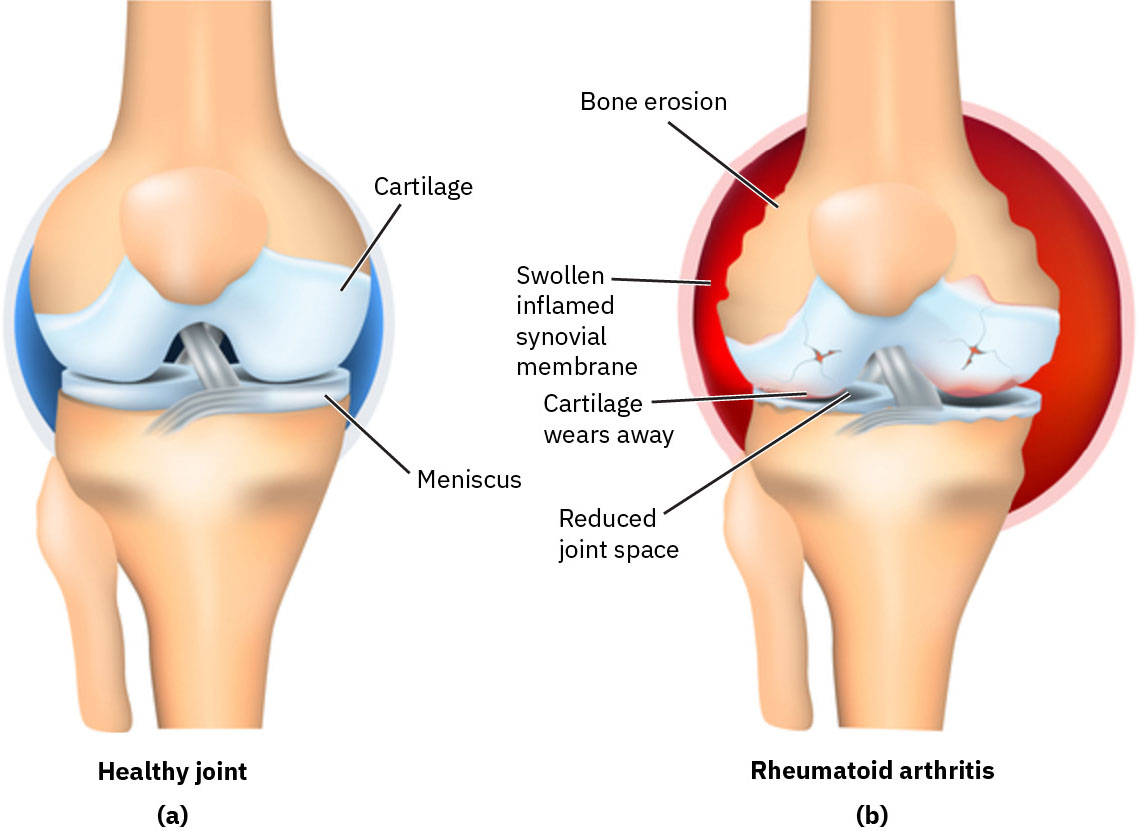 Illustration reference: OpenStax Clinical Nursing Skills Ch.25.
Illustration reference: OpenStax Clinical Nursing Skills Ch.25.
RA is an immune-mediated inflammatory condition in which the body attacks synovial membranes. Persistent synovial inflammation damages cartilage, bone, and nearby structures, producing chronic pain and progressive joint dysfunction. In genetically susceptible individuals, environmental triggers such as cigarette smoking or asbestos exposure may contribute to autoantibody activation and inflammatory-joint destruction.
The inflammatory process is commonly bilateral and involves multiple joints, especially hands and wrists. Over time, untreated inflammation leads to instability, reduced range of motion, muscle wasting from disuse, and characteristic deformities.
Classification
- Early-stage RA: Joint tenderness, warmth, swelling, fatigue, and morning stiffness lasting more than 30 minutes.
- Late-stage RA: Severe deformities (including swan-neck or boutonniere patterns), contractures, instability, and advanced functional loss.
- Systemic RA involvement: Extra-articular effects may include pleuritic symptoms, neuropathic findings, and inflammatory eye complications.
Risk Factors
- Female sex and typical onset in early-to-mid adulthood.
- Female prevalence is about two times that of male prevalence in many cohorts.
- Family history and genetic susceptibility.
- Chronic stress burden that may amplify immune dysregulation.
- Environmental exposures (for example cigarette smoking and asbestos exposure) can increase risk in genetically predisposed individuals.
Nursing Assessment
NCLEX Focus
Prioritize recognition of inflammatory versus degenerative joint patterns and monitor for function-limiting progression.
- Assess bilateral joint pain, swelling, erythema, warmth, and prolonged morning stiffness.
- Assess for rheumatoid nodules, especially around pressure areas and extensor surfaces.
- Assess bilateral grip strength and functional hand use because hand-joint involvement is common and often disabling.
- In hand-dominant presentations, assess bilateral MCP/PIP tenderness, edema, erythema, and pain-limited finger ROM.
- Differentiate RA from osteoarthritis patterns: RA is typically inflammatory and symmetric, whereas OA is more wear-related and often less symmetric early in disease.
- Assess function and mobility, including range of motion, gait limitations, fatigue burden, and ADL impact.
- Assess for constitutional flare cues (for example low-grade fever, malaise, anorexia, and unusual fatigue) that may precede or accompany inflammatory joint worsening.
- Monitor for deformity progression, including swan-neck and boutonniere changes, and for contracture development.
- Review diagnostic trends supporting inflammatory autoimmune disease, including RF, ANA, ESR, and CRP.
- During palpation, document boggy joint texture when present because it supports active inflammatory synovitis.
- Recognize that RF is present in a large proportion of RA cases (about 90% in cohorts), but interpretation should be integrated with clinical and inflammatory-marker context.
- Use imaging (x-ray, ultrasound, MRI) to assess erosive damage, while recognizing that early-stage RA can have normal imaging and should not be ruled out by imaging alone.
- In pregnancy-capable patients, assess current RA medication safety and reinforce early reporting of worsening fatigue, joint pain, or swelling.
- Assess for extra-articular findings and infection risk when immunosuppressive or biologic therapy is used.
Stage-Pattern Findings
- Early RA:
- Symmetric multi-joint pain/tenderness with warmth and erythema.
- Morning stiffness lasting more than 30 minutes.
- Fatigue and muscle weakness.
- Possible mild pleuritic symptoms, pericardial friction rub, neuropathic paresthesia, or eye dryness/irritation.
- Late RA:
- Advanced deformity, contractures, instability, limited ROM, and disuse muscle wasting.
- Increased cardiovascular risk (accelerated atherosclerotic burden).
- Pleurisy/interstitial-lung-disease progression risk.
- Peripheral neuropathy and inflammatory eye involvement (for example scleritis).
Nursing Interventions
- Use structured pain reassessment with pharmacologic and nonpharmacologic strategies such as heat, cold, relaxation, and activity pacing.
- Reinforce joint-protection techniques, proper use of splints or braces, and routine skin checks at pressure-risk sites.
- Support physical and occupational therapy plans to preserve flexibility, strength, and independent function.
- Coordinate medication plans that combine DMARD, NSAID, and corticosteroid pathways as ordered, and reinforce taper adherence when steroid reduction is planned.
- Reinforce alternating rest and activity periods to reduce inflammatory-joint stress without complete deconditioning.
- Teach energy-conservation methods and adaptive equipment use for home and work routines.
- For pregnancy planning or active pregnancy, coordinate medication-review counseling and high-risk obstetric referral as indicated.
- Provide infection-prevention education for immune-suppressing therapy, including hygiene, vaccine updates, exposure avoidance, and early symptom reporting.
- Monitor and protect skin integrity over nodules or brace/splint pressure points.
Infection-Prevention Teaching Under Immunosuppression
- Reinforce consistent hand hygiene and personal hygiene routines.
- Avoid close exposure to symptomatic ill contacts.
- Maintain recommended vaccinations in coordination with the care team.
- Use safe food-handling practices to reduce foodborne infection risk.
- Limit exposure to crowded outbreak settings when possible.
- Use protective equipment as indicated in health care or high-risk public settings.
- Maintain household environmental hygiene and routine surface disinfection.
- Report infection symptoms promptly and maintain active communication with providers.
Advocacy and Psychosocial Support
- Coordinate multidisciplinary RA care (nursing, rheumatology, PT, OT, and other specialists as needed).
- Address treatment-access barriers and support self-management planning.
- Reinforce joint protection, energy conservation, and independence-focused assistive-device use.
- Use therapeutic communication for chronic-illness distress and encourage support-group/community-resource engagement.
Common Nursing Diagnoses
- Chronic pain.
- Impaired mobility.
- Fatigue.
- Risk for altered skin integrity.
Outcome Indicators
- Pain level reduced to personalized target (for example ⇐ 3/10) in planned timeframe.
- Correct performance of prescribed exercise and mobility-support techniques.
- Reduced fatigue burden with improved ADL participation.
- Intact skin over high-risk pressure/nodule areas.
- Improved ROM, lower swelling/stiffness burden, and stronger grip function on follow-up assessment.
- No significant medication adverse effects reported during treatment monitoring.
High-Risk Immunosuppressive Therapy Effects
DMARDs and biologics can cause severe adverse reactions and infection vulnerability, requiring close monitoring and rapid escalation of concerning findings.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| nsaids | ibuprofen, naproxen | Improve pain and inflammation; monitor response and tolerability. |
| analgesics | acetaminophen, selected opioid use | Symptom-control adjuncts; reassess benefit-risk and function outcomes. |
| corticosteroids | prednisone, intra-articular corticosteroid | Short-term flare control; monitor for adverse effects (for example weight gain, osteoporosis, infection risk) and taper carefully to reduce adrenal-insufficiency risk. |
| disease-modifying-antirheumatic-drugs (antimalarial agents) | hydroxychloroquine, chloroquine | Used for inflammatory symptom control and flare reduction in selected plans. |
| immunosuppressants | cyclophosphamide in severe-case contexts | Reserve for high-severity disease; monitor toxicity and infection risk closely. |
| disease-modifying-antirheumatic-drugs | methotrexate, sulfasalazine | Slow disease progression; methotrexate is contraindicated in pregnancy and requires preconception medication review. |
| biologic-response-modifiers | class-based biologics | Target immune pathways; monitor closely for infection risk. |
| biologic-response-modifiers (tumor necrosis factor inhibitors) | infliximab, adalimumab | Reduce inflammatory activity; caution when active or serious infection risk exists. |
Clinical Judgment Application
Clinical Scenario
A middle-aged client reports bilateral hand pain, prolonged morning stiffness, fatigue, and worsening difficulty with dressing and meal preparation, with elevated inflammatory markers.
- Recognize Cues: Symmetric inflammatory joint findings with functional decline.
- Analyze Cues: Pattern supports active autoimmune synovitis with progression risk.
- Prioritize Hypotheses: Highest priority is limiting joint damage while preserving independence and safety.
- Generate Solutions: Optimize pain control, reinforce therapy participation, and strengthen self-management education.
- Take Action: Implement mobility and skin/joint protection plan, monitor medication effects, and escalate worsening findings.
- Evaluate Outcomes: Pain decreases, daily function improves, and no new deformity progression is observed.
Evaluation
- Reassess outcomes as met, partially met, or unmet within the stated time goals.
- Revise care plan when symptom control, mobility, fatigue, or skin goals are not achieved.
- Re-evaluate after interventions, updated diagnostics/labs, and interprofessional care-plan reviews.
Related Concepts
- common-musculoskeletal-disorders-recognition-and-care-priorities - Differential pattern recognition across chronic joint disorders.
- fall-prevention - Mobility decline and weakness increase fall and injury risk.
- kidney-disease - Comorbidity and medication-safety context in chronic disease management.
- activities-of-daily-living - RA symptom burden often reduces independent self-care performance.
- trauma-informed-care - Chronic pain and disability require supportive, person-centered communication strategies.
Self-Check
- Which findings best differentiate early inflammatory RA from late structural RA damage?
- Why are DMARDs prioritized even when short-term pain control improves symptoms?
- Which teaching points most reduce infection risk during biologic or other immunosuppressive therapy?