Ventilator Waveform Interpretation
Key Points
- Waveform analysis is essential immediately after mechanical ventilation initiation to verify patient demand matching and synchrony.
- Reduced compliance and increased resistance create distinct waveform behavior and altered filling dynamics.
- Auto-PEEP and double triggering are high-yield waveform findings linked to complications and patient-ventilator asynchrony.
- Unsafe waveform patterns can signal risk for barotrauma, volutrauma, and hypotension.
Pathophysiology
Ventilator graphics visualize dynamic interactions between machine-delivered breath mechanics and patient respiratory system behavior. Changes in compliance, resistance, inspiratory timing, and patient effort alter pressure, flow, and volume waveforms before overt clinical instability appears.
When compliance decreases, the lungs accept less volume and can fill more quickly at smaller capacity. When airway resistance increases, airflow through the airways is reduced and more time is needed to deliver target tidal volume. Misalignment between neural respiratory drive and ventilator timing can produce waveform-detectable asynchrony patterns, including active exhalation against ongoing inspiratory time or double triggering.
Classification
- Compliance-related waveform change: Lower accepted volume with altered curve shape compared with normal conditions.
- Resistance-related waveform change: Slower filling dynamics and prolonged time required for volume delivery.
- Auto-PEEP pattern: Persistent expiratory flow with expiratory-pause pressure estimate indicating trapped pressure.
- Asynchrony patterns: Active exhalation during inspiratory phase and double triggering from ongoing inspiratory effort.
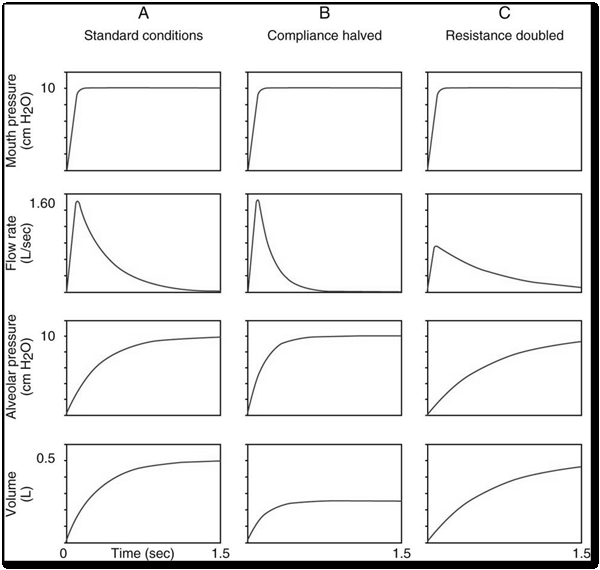 Illustration reference: OpenRN Respiratory Therapy Ch.5.1.
Illustration reference: OpenRN Respiratory Therapy Ch.5.1.
Nursing Assessment
NCLEX Focus
Priority questions often ask which waveform pattern indicates asynchrony and which adjustments reduce injury risk.
- Assess pressure/flow/volume waveforms after ventilation starts and after each setting change.
- Identify signs of auto-PEEP and estimate intrinsic pressure contribution using expiratory pause context.
- Watch for double triggering or active exhalation signatures that suggest timing mismatch.
- Correlate waveform findings with hemodynamics and gas-exchange changes.
Nursing Interventions
- Escalate waveform abnormalities early to respiratory therapy and provider team.
- Support mode/parameter optimization when I-time appears too long for patient exhalation needs.
- Monitor for complications associated with elevated mean airway pressures, including hypotension and pressure injury risk.
- Reinforce ongoing waveform surveillance during transport, sedation changes, and clinical instability.
- Document waveform findings and response to adjustments for trend continuity.
Hidden Injury Risk
Unrecognized auto-PEEP and asynchrony can increase pressure-related injury and destabilize cardiopulmonary status.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| sedative-hypnotics | Synchrony-support context | Sedation level affects trigger behavior and waveform synchrony; monitor for over- and under-sedation effects. |
| bronchodilators | Resistance-reduction context | Airflow improvement may reduce resistance-related waveform abnormalities in selected patients. |
Clinical Judgment Application
Clinical Scenario
A ventilated patient develops closely spaced paired breaths with pressure drops during inspiratory phase and rising concern for discomfort.
- Recognize Cues: Pattern suggests double triggering and patient-ventilator mismatch.
- Analyze Cues: Inspiratory time and trigger interaction may be misaligned with patient effort.
- Prioritize Hypotheses: Immediate priority is reducing asynchrony and preventing pressure-related harm.
- Generate Solutions: Reassess timing/trigger strategy, evaluate auto-PEEP contribution, and adjust support plan.
- Take Action: Communicate findings and implement ordered ventilator optimization.
- Evaluate Outcomes: Waveforms normalize, synchrony improves, and patient distress decreases.
Related Concepts
- invasive-mechanical-ventilation-modes - Mode behavior determines baseline waveform expectations.
- ventilator-parameter-adjustment-principles - Adjustment strategy should follow waveform-informed oxygenation/ventilation goals.
- pressure-control-ventilation-monitoring - Continuous trend interpretation is central to safe pressure-targeted support.
- psv-and-simv-setup-verification - Set-versus-observed tracking supports accurate waveform interpretation.
- respiratory-failure - Severe gas-exchange compromise increases susceptibility to asynchrony and pressure complications.
Self-Check
- How do reduced compliance and increased resistance produce different waveform changes?
- Why does auto-PEEP increase risk of hypotension and pressure injury?
- What waveform cues should trigger immediate reassessment of inspiratory timing and synchrony?