Care in the Second Trimester of Pregnancy
Key Points
- Second-trimester visits continue risk surveillance while fetal assessment becomes more detailed.
- Fundal height, fetal heart rate, and fetal movement trends are key routine assessments.
- Midpregnancy labs and anatomy ultrasound detect evolving maternal-fetal risk.
- Education emphasizes warning signs that differ from first-trimester patterns.
- Common timing checkpoints include anatomy ultrasound around 16 to 20 weeks and gestational-diabetes screening around 24 to 28 weeks.
- High-risk second-trimester complications include abortion pathways, cervical-insufficiency, and Rh-alloimmunization risk.
Pathophysiology
During the second trimester (about 14 weeks through 27 weeks and 6 days), fetal growth accelerates and maternal adaptation continues. Many symptoms improve, but new risk pathways emerge, including preterm labor signals, hypertensive patterns after 20 weeks, and glycemic dysregulation.
Because symptom meaning shifts with gestational age, the same complaint can represent different risks than in earlier pregnancy. Ongoing interval assessment and trend-based interpretation prevent delayed detection.
Classification
- Routine surveillance domain: Interval history, vitals, edema, fundal height, and fetal heart monitoring.
- Laboratory domain: Integrated/quad screening, anemia monitoring, glucose screening, and Rh-related testing.
- Imaging domain: Anatomy ultrasound and placental/fetal growth assessment.
- Education domain: Midpregnancy warning-sign and self-monitoring reinforcement.
- High-risk complication domain: Midtrimester abortion, cervical dilation insufficiency, and Rh-immunohematologic risk pathways.
Nursing Assessment
NCLEX Focus
Evaluate symptom context by gestational age and trend, not as isolated complaints.
- Obtain interval history for bleeding, fluid leakage, contractions/cramping, headache, visual change, edema, and reduced fetal movement.
- Treat persistent vomiting, dysuria with intermittent back pain, recurrent dizziness/syncope, persistent abdominal or epigastric pain, and visual changes as escalation cues in second-trimester follow-up.
- If interval weight trend is lower or higher than expected (or weight loss occurs), perform 24-hour diet recall and appetite-change review.
- Measure fundal height and compare with gestational-age expectation.
- From about 16 to 18 weeks through 36 weeks, expect fundal height in centimeters to approximate gestational age in weeks.
- Use landmarks to cross-check trend: fundus is typically halfway between symphysis and umbilicus at 16 weeks and near the umbilicus by 20 weeks.
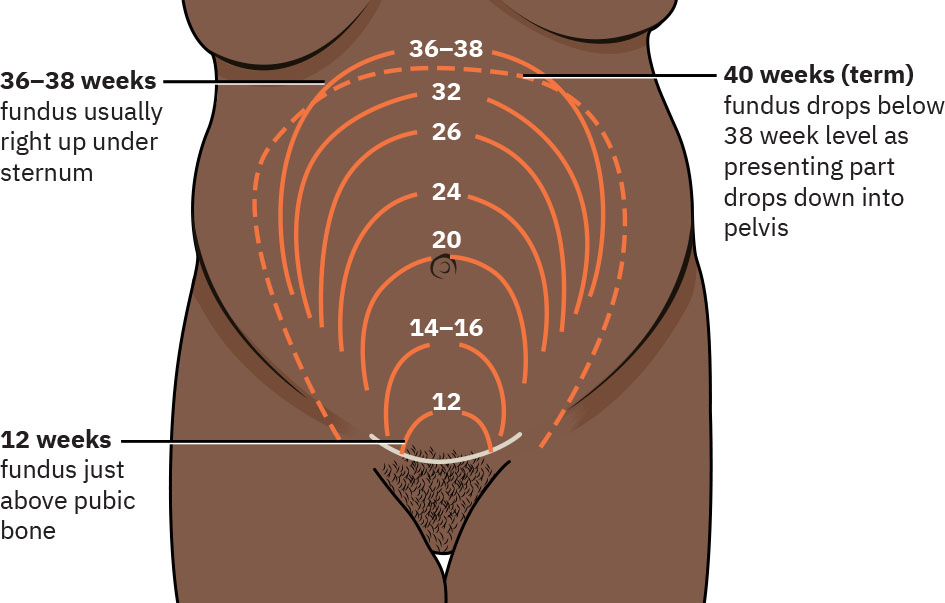 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.11.3.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.11.3.
- Auscultate fetal heart rate and rhythm; assess movement pattern changes.
- Treat fetal heart rate of 110 to 160 bpm as expected baseline and escalate persistent deviation.
- Recognize that fetal heart tones best heard low in the maternal abdomen suggest cephalic presentation, while tones best heard high can suggest breech presentation.
- Expect quickening to begin around 16 to 24 weeks and increase over time in uncomplicated pregnancies.
- Teach that multiparous patients may perceive quickening earlier than primiparous patients.
- Review lab/imaging results and identify abnormal follow-up needs.
- Report BP findings in gestational context: BP at or above 140/90 before 20 weeks supports preexisting hypertension concern, while new BP elevation/proteinuria after 20 weeks increases concern for preeclampsia.
- Treat positive urine nitrites as possible UTI requiring further clinical evaluation.
- Review second-trimester CBC trend for anemia and thrombocytopenia risk signals (including platelet decline from baseline).
- Escalate hemoglobin below about 10.5 g/dL in second trimester as likely iron-deficiency-anemia pathway requiring treatment review.
- Escalate significant platelet decline from baseline or platelet count below about 150,000/uL as possible hypertensive/liver-complication cue.
- Screen for social and access barriers that affect adherence.
Nursing Interventions
- Reinforce nutrition, activity, hydration, and symptom self-monitoring.
- Reinforce expected routine visit cadence of about every 4 weeks in uncomplicated second-trimester care.
- Use gestational-context teaching: before 20 weeks, cramping/bleeding can indicate miscarriage; after 20 weeks, similar symptoms increase concern for preterm labor. Edema before 20 weeks may indicate underlying cardiac disease, while edema after 20 weeks raises concern for hypertensive disorder.
- Reinforce fetal-milestone teaching in plain language, including quickening trends and viability context around 23 to 24 weeks as surfactant production begins.
- Use weight trend as a nutrition-access screen: investigate weight loss for illness or food insecurity and evaluate rapid gain for fluid retention or low activity patterns.
- Explain purpose and limits of screening tests (risk stratification versus diagnosis).
- Reinforce timing of key second-trimester tests (anatomy ultrasound about 16 to 20 weeks; gestational-diabetes screening about 24 to 28 weeks).
- Coordinate additional testing or specialist referral for abnormal findings.
- Clarify when to call urgently versus when routine follow-up is appropriate.
- Maintain continuity documentation for third-trimester transition planning.
Gestational-Context Miss
Treating second-trimester warning symptoms as first-trimester “normal” can delay preterm or hypertensive care.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| anemia-overview-and-transfusion-thresholds (iron-supplementation) | iron-deficiency-anemia (Iron-deficiency anemia) treatment contexts | Used when second-trimester hemoglobin trends indicate deficiency. |
| rh-immune-globulin | Rh-negative pregnancy prophylaxis contexts | Administered per protocol to reduce alloimmunization risk. |
Clinical Judgment Application
Clinical Scenario
A 24-week patient reports persistent headache, visual blurring, and new hand swelling after previously normal visits.
- Recognize Cues: Symptom cluster is concerning after 20 weeks.
- Analyze Cues: Pattern may signal hypertensive disorder rather than routine discomfort.
- Prioritize Hypotheses: Immediate maternal-fetal risk evaluation is priority.
- Generate Solutions: Escalate assessment, obtain targeted labs/vitals, and provider review.
- Take Action: Initiate urgent triage pathway.
- Evaluate Outcomes: Complication is identified or excluded promptly.
Related Concepts
- care-in-the-first-trimester-of-pregnancy - Early baseline findings inform second-trimester interpretation.
- care-in-the-third-trimester-of-pregnancy - Midpregnancy trends guide late-pregnancy surveillance intensity.
- cervical-insufficiency - Painless cervical dilation in midpregnancy requires urgent escalation planning.
- fetal-growth-and-development - Anatomy and growth milestones shape second-trimester testing.
- physiologic-changes-due-to-pregnancy - Normal adaptation patterns help avoid over/under-triage.
- person-and-family-centered-care - Education should align with patient goals and context.
Self-Check
- Which second-trimester symptoms require same-day escalation?
- How do screening and diagnostic tests differ in counseling language?
- Why is fundal-height trend more useful than a single measurement?