Fetal Growth and Development
Key Points
- Development progresses through pre-embryonic, embryonic, and fetal stages with stage-specific vulnerability windows.
- Organogenesis is the highest-risk period for major structural malformations from teratogenic exposure.
- Placenta and fetal membranes are central to gas, nutrient, waste, and hormonal support.
- Nursing counseling should integrate genetics, environment, infection, and lifestyle influence on fetal outcomes.
Pathophysiology
Fetal development begins with fertilization, cleavage, and implantation, followed by germ-layer differentiation and organogenesis. During embryonic development (about day 16 through week 8 postconception), foundational organ structures form; during fetal development, growth and functional maturation predominate.
In early pre-embryonic progression, the zygote divides to a morula stage (about 16 cells), typically reaching the uterus in roughly 72 hours. Cell-line specialization then forms blastocyst tissue (future embryo and amnion) and trophoblast tissue (future placenta and chorion). Implantation generally occurs when trophoblast tissue attaches to endometrium about 7 to 10 days after conception, and the full pre-embryonic sequence is commonly described as about 10 to 14 days.
The embryonic stage begins after implantation and continues to the start of gestational week 9, with organogenesis driven by ectoderm, mesoderm, and endoderm differentiation. Obstetric gestational timing is counted from the first day of the last menstrual period rather than conception date.
Placental formation creates a selective exchange interface between maternal and fetal circulations without direct blood mixing. Placental hormones sustain pregnancy, influence maternal metabolism, and support fetal growth. Fetal circulation and amniotic systems enable oxygen delivery, movement, temperature stability, and developmental protection. Structurally, fetal chorionic-villi vasculature interfaces with maternal decidua basalis tissue to form placental lobes (cotyledon architecture) and umbilical-cord vascular pathways, and gross placental formation is typically complete around week 12.
Placental transport functions include respiratory gas exchange (oxygen to fetus, carbon dioxide to parent), nutrient transfer (glucose diffusion, amino-acid active transport, fatty-acid diffusion, water/electrolyte diffusion, and active transfer of selected micronutrients such as iron/calcium/vitamins), and fetal waste handling (for example urea, uric acid, bilirubin transfer for maternal elimination). Hormonal output includes progesterone, estrogen, hCG, hPL, and relaxin.
Fetal membranes (chorion and amnion) and amniotic fluid provide infection buffering, movement freedom, cushioning, and thermal stability. Amniotic-fluid production is initially membrane-driven, then increasingly kidney-driven as fetal renal function matures.
Exposure timing strongly determines outcome: early teratogenic exposures can cause major malformations; later exposures often affect growth, function, or neurodevelopment. During organogenesis, short windows of structural separation (for example early trachea-esophagus partitioning) are especially vulnerability-sensitive. Nutritional and medication exposures are high-yield counseling targets: folate deficiency is linked to neural-tube-defect patterns, while excess vitamin A exposure (for example isotretinoin pathways) is associated with serious craniofacial malformation risk.
Early week-by-week embryonic milestones include neural-tube and limb-bud development in week 3, expanding brain and visceral primordia by week 4, detectable cardiac activity around week 5, and established fetal circulation with rapid CNS/organ progression by week 6. By weeks 7 to 8, coordinated movement patterns, facial development, and ongoing skeletal and organ maturation continue.
Key fetal-period milestones include first perceived movement (quickening) around 16 to 24 weeks, increasing survival potential near 23 to 24 weeks with intensive neonatal support, and progressive organ maturation toward term. By about 37 weeks, most organ systems are sufficiently developed for extrauterine survival with substantially lower prematurity risk than earlier gestations. Gonadal differentiation often occurs by about 8 weeks, and testicular descent typically occurs around 34 to 36 weeks. Abdominal-wall closure vulnerability around about 10 weeks is clinically relevant because teratogen-linked disruption can contribute to defects such as gastroschisis or omphalocele.
Additional timing cues used in prenatal teaching include early ossification and fetal urine production around 12 weeks, meconium formation around 16 weeks, and progressive viability physiology around 24 weeks as alveoli and surfactant production begin. Digestive-enzyme maturity remains limited until later gestation (around 36 weeks), which contributes to preterm feeding vulnerability.
Fetal circulation uses three major shunts to bypass nonfunctioning lungs before birth: ductus venosus, foramen ovale, and ductus arteriosus. Oxygenated placental blood returns by umbilical vein, and deoxygenated blood returns to placenta by umbilical arteries. After birth, pulmonary expansion and cord clamping trigger transitional closure of these pathways (foramen ovale functionally first, ductus arteriosus typically within about 24 to 48 hours, and ductus venosus collapse after cord flow stops).
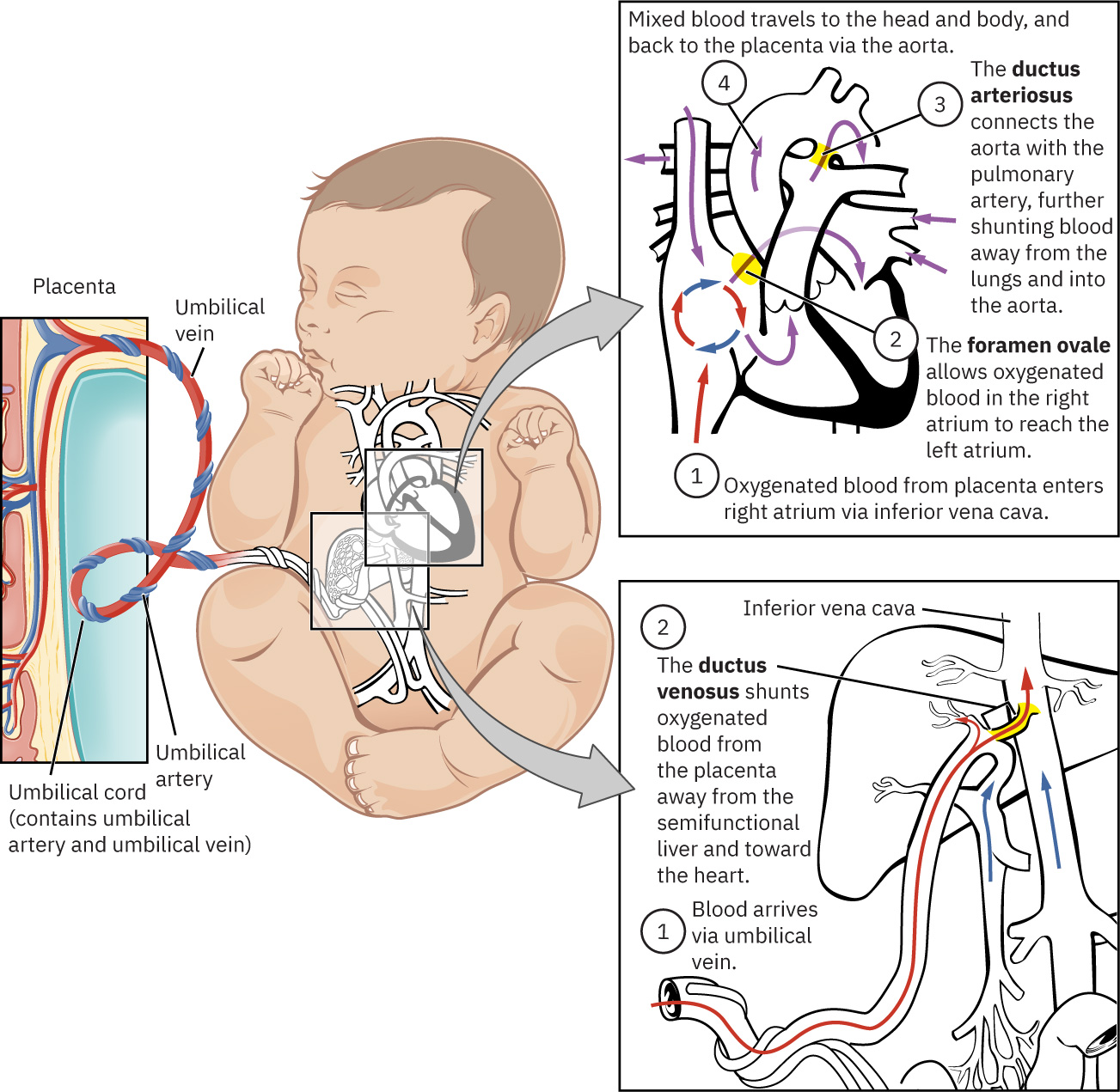 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.10.4.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.10.4.
Classification
- Development stages: Pre-embryonic (implantation), embryonic (organogenesis), fetal (growth and maturation).
- Embryonic milestone domains: Week-by-week organ primordia and early system-function onset (for example heartbeat, neural tube/CNS progression, limb/facial development).
- Fetal milestone domains: Quickening, hearing responsiveness, late-third-trimester growth acceleration, and transition from preterm vulnerability to near-term readiness.
- Support systems: Placenta, amnion/chorion, amniotic fluid, and umbilical circulation.
- Risk-influence domains: Genetics, chromosomal abnormalities, infections, chemicals/drugs, nutrition, and chronic disease.
- Outcome domains: Structural anomalies, growth restriction, functional deficits, and pregnancy loss.
Nursing Assessment
NCLEX Focus
Prioritize timeline-based risk assessment: what exposure happened, when it occurred, and which organs were developing then.
- Assess preconception and prenatal exposure history (medications, substances, infections, occupational/environmental hazards).
- Review family/genetic history and need for counseling/testing pathways.
- Track gestational-age milestones and expected fetal growth patterns.
- Evaluate maternal conditions affecting fetal development (diabetes, nutrition deficits, hypertensive disease).
- Screen for access barriers to consistent prenatal surveillance.
Nursing Interventions
- Provide trimester-specific counseling on developmental milestones and vulnerability windows.
- Reinforce folate, balanced nutrition, and avoidance of known teratogens.
- Coordinate indicated genetic counseling and diagnostic follow-up.
- Educate on infection prevention and timely treatment in pregnancy.
- Support informed decision-making with clear, non-coercive communication.
Exposure-Timing Oversight
Ignoring gestational timing of exposures can misclassify fetal risk and delay needed evaluation.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| prenatal-vitamins | Folic acid and micronutrient support contexts | Critical for neural-tube risk reduction and baseline fetal growth support. |
| preconception-teratogen-and-medication-exposure-review (teratogenic-medications) | Isotretinoin and related high-risk agents | Require strict avoidance/counseling and immediate provider review if exposure occurs. |
Clinical Judgment Application
Clinical Scenario
A patient learns they used a known teratogenic acne medication in early first trimester before recognizing pregnancy.
- Recognize Cues: Exposure occurred during high-vulnerability organogenesis window.
- Analyze Cues: Risk level depends on agent dose, timing, and specific organ development stage.
- Prioritize Hypotheses: Priority is urgent maternal-fetal medicine and genetics referral.
- Generate Solutions: Arrange targeted counseling, imaging/diagnostic timeline, and supportive decision resources.
- Take Action: Document exposure details and coordinate expedited follow-up.
- Evaluate Outcomes: Patient receives accurate risk stratification and ongoing surveillance plan.
Related Concepts
- fertility-and-conception - Conception sequence establishes developmental starting point and implantation success.
- genetics-in-reproductive-care - Inheritance and chromosomal risk shape developmental outcomes.
- physiologic-changes-due-to-pregnancy - Maternal adaptations sustain placental and fetal growth demands.
- preconceptual-care - Early risk reduction has highest developmental impact before/early in pregnancy.
- person-and-family-centered-care - Counseling should align with family values and informed choices.
Self-Check
- Why is organogenesis the most critical period for teratogenic harm?
- Which maternal factors most strongly alter fetal growth and developmental trajectory?
- How should nurses explain placental function without oversimplifying maternal-fetal exchange?