Anemia Overview and Transfusion Thresholds
Key Points
- Anemia reflects reduced red blood cell count, hemoglobin, or hematocrit, causing reduced oxygen delivery to tissues.
- Common manifestations include fatigue, weakness, pallor, dyspnea, and palpitations.
- Severe symptomatic anemia can progress to syncope, angina, or myocardial infarction.
- Common anemia mechanisms include reduced RBC production, blood loss, nutritional deficiency, and accelerated RBC destruction.
- WHO anemia staging varies by age and pregnancy status; severe anemia is commonly below 8 g/dL in most older child/adult groups.
- Restrictive transfusion thresholds commonly use hemoglobin 7 g/dL or less for stable hospitalized adults and 8 g/dL or less for selected higher-risk surgical/cardiovascular populations.
- In severe symptomatic or actively bleeding cases, transfusion decisions are individualized; when not actively bleeding, one-unit PRBC strategy with reassessment is commonly used.
Pathophysiology
Anemia is an abnormal oxygen-transport state rather than a single disease entity. It develops when red cell mass, hemoglobin concentration, or hematocrit falls enough to reduce oxygen delivery to organs. Because multiple etiologies can produce this pattern, diagnosis and management are cause-directed rather than one-size-fits-all.
Reduced RBC production can occur with bone marrow dysfunction or reduced Erythropoietin signaling in kidney disease. Other common routes include acute or chronic blood loss, nutrient deficiency (especially iron, vitamin B12, and folate), and Hemolysis with destruction outpacing marrow replacement.
As tissue oxygen supply declines, compensatory cardiovascular responses occur, including increased heart rate and subjective palpitations. In more severe states, oxygen mismatch can trigger ischemic symptoms such as chest pain and may contribute to myocardial injury.
Classification
- Production-deficit anemia: Reduced marrow output or low erythropoietin response.
- Loss-related anemia: Acute hemorrhage or chronic occult blood loss.
- Nutritional-deficit anemia: Iron, B12, or folate depletion.
- Inflammation-related functional iron deficiency: Iron stores may be present but unavailable to erythroid precursors (common in chronic inflammatory/cancer pathways).
- Hemolytic anemia: Accelerated RBC destruction.
Diagnostic Pattern Recognition
- WHO hemoglobin cut points vary by age and pregnancy status; in many adult/older-child groups, severe anemia is below about 8 g/dL.
- Hemogram interpretation uses RBC quantity plus red-cell indices such as MCV and MCHC.
- Common index patterns include microcytic (MCV low), macrocytic (MCV high), and normocytic/normochromic patterns, each narrowing differential diagnosis.
Nursing Assessment
NCLEX Focus
Prioritize recognition of inadequate oxygen delivery and identify when anemia findings require urgent escalation.
- Assess for fatigue, generalized weakness, pallor, dyspnea, and palpitations.
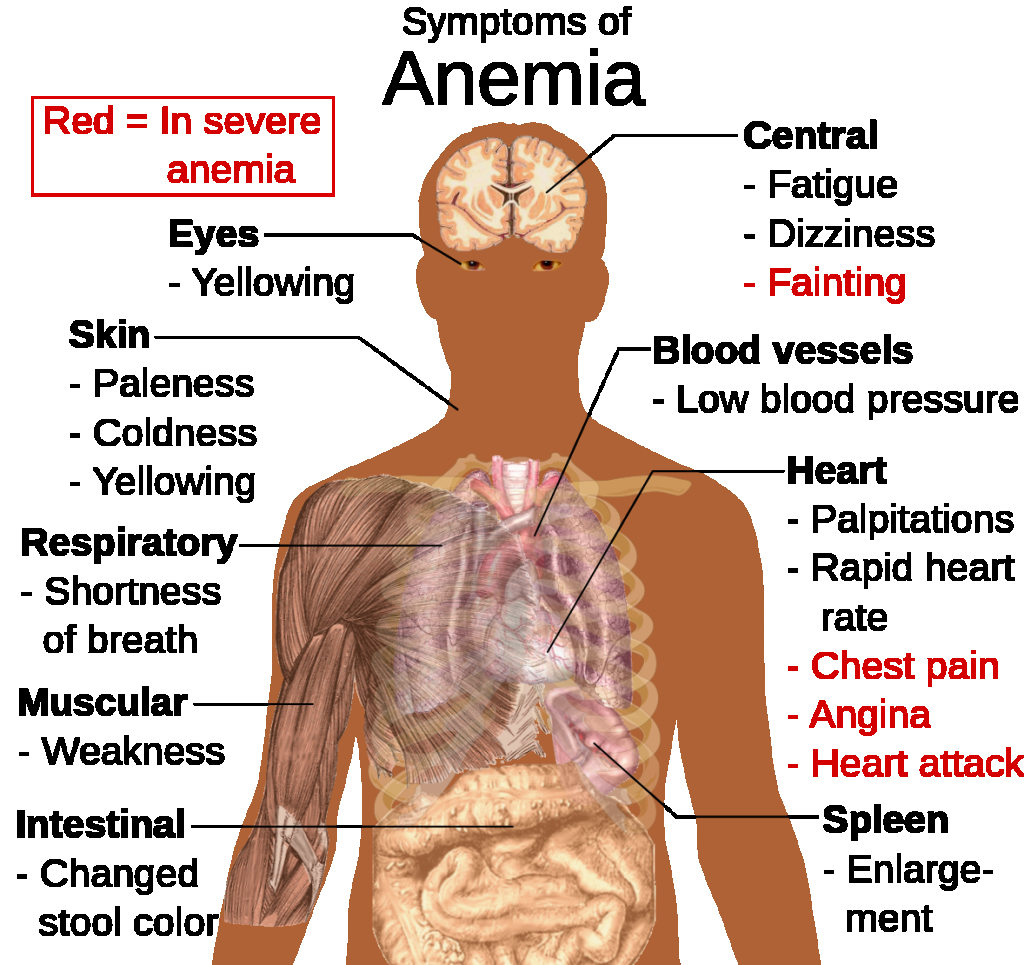 Illustration reference: OpenRN Health Alterations Ch.3.5.
Illustration reference: OpenRN Health Alterations Ch.3.5.
- Assess for nutrition-linked anemia cues such as pica, poor diet diversity, and inadequate intake of iron, folate, vitamin B12, copper, vitamin C, and vitamin E.
- Assess perfusion-focused objective findings such as delayed capillary refill, tachycardia, hypotension, and hypoxemia trend.
- In severe symptom patterns, monitor for ECG changes/tachyarrhythmia as signs of escalating oxygen-delivery strain.
- Escalate severe manifestations such as fainting, chest pain, or signs of cardiac ischemia.
- Review common adult etiologies including GI blood loss, kidney-disease, and excessive menstrual blood loss.
- In oncology contexts, assess for multifactorial drivers such as chronic inflammation, treatment effects, poor intake/anorexia, and GI blood loss.
- Trend hemoglobin/hematocrit and correlate with symptoms to determine clinical severity.
- Screen for bleeding cues including easy bruising, melena, hematuria, epistaxis, or heavy menstrual bleeding.
- Include dietary pattern and absorption-risk assessment for iron/B12/folate deficiency.
- Do not rely on pulse oximetry alone in severe anemia because SpO2 may appear normal despite clinically significant oxygen-delivery deficit.
Nursing Interventions
- Support targeted treatment of underlying causes after diagnostic evaluation.
- Implement oxygenation and activity-tolerance support strategies while definitive treatment is organized.
- For severe symptomatic anemia or hemoglobin below 7 g/dL, prepare for blood-transfusion-verification-initiation-and-reaction-response per protocol.
- For orthopedic/cardiac surgery or preexisting cardiovascular disease contexts, recognize that transfusion may be considered at hemoglobin 8 g/dL or less based on condition and symptoms.
- Unless active hemorrhage is present, use single-unit PRBC transfusion with post-unit clinical and laboratory reassessment before additional units.
- Apply fall precautions and pace activity with clustered care plus planned rest when weakness is prominent.
- Monitor for ongoing blood loss with serial hemoglobin/hematocrit trends, stool/urine bleeding surveillance, and drain-output review when applicable.
- Monitor clinical response after intervention, including symptoms and follow-up hemoglobin trends.
- Support blood-bank policy that standard-issue RBC units are acceptable unless a specific order/indication requires a different product profile.
High-Acuity Progression
Chest pain, syncope, or worsening dyspnea in anemia can indicate critical oxygen-delivery compromise and requires immediate provider notification.
Clinical Judgment Application
Clinical Scenario
An adult with progressive fatigue and dyspnea has pallor, palpitations, and a hemoglobin level below 7 g/dL.
- Recognize Cues: Symptoms and laboratory findings indicate significant oxygen-transport deficit.
- Analyze Cues: Severity raises risk for cardiopulmonary compromise.
- Prioritize Hypotheses: Immediate problem is severe symptomatic anemia.
- Generate Solutions: Escalate promptly, prepare transfusion workflow, and monitor closely.
- Take Action: Initiate protocol-based transfusion preparation and surveillance.
- Evaluate Outcomes: Symptoms stabilize and hemoglobin improves toward target range.
Related Concepts
- iron-deficiency-anemia - Common microcytic cause of reduced oxygen-carrying capacity.
- vitamin-b12-and-folate-deficiency-anemia - Megaloblastic anemia patterns with distinct treatment needs.
- aplastic-anemia-pancytopenia-management - Marrow-failure mechanism of anemia with additional cytopenias.
- blood-transfusion-verification-initiation-and-reaction-response - Safety-critical transfusion workflow in severe symptomatic cases.
- cbc - Hemogram indices (MCV/MCHC) support anemia pattern classification.
- hemostasis-coagulation-and-fibrinolysis - Bleeding-related anemia risk intersects with clotting and hemorrhage control.
Self-Check
- Why is anemia considered a clinical condition rather than one single disease?
- Which findings suggest progression from mild anemia to high-acuity oxygen-delivery compromise?
- When is packed red blood cell transfusion commonly considered in severe anemia?