Meningitis Priority Care and ICP Risk
Key Points
- Meningitis is inflammatory infection of the meninges and can rapidly become life-threatening.
- Common bacterial causes include Streptococcus pneumoniae and Neisseria meningitidis, while viral causes are often self-limited.
- Bacterial meningococcal meningitis is a medical emergency; untreated mortality can approach 50%, and severe outcomes can occur even with treatment.
- Priority risks are increased intracranial pressure (ICP), neurologic injury, seizures, and brain herniation.
- Early antibiotics, corticosteroids, neurologic monitoring, and transmission precautions are core nursing priorities.
- High-severity progression can include brain injury plus hearing/vision loss, requiring early escalation and follow-up planning.
Pathophysiology
Meningitis is an infectious inflammatory process involving the membranes surrounding the brain and spinal cord. Infection may spread hematogenously from other sites or occur by direct transmission after local infection, trauma, or invasive procedures.
The meninges are composed of the pia mater, arachnoid mater, and dura mater. Inflammation within or adjacent to these spaces, particularly where cerebrospinal fluid circulates in the subarachnoid space, contributes to edema, pain, and neurologic compromise.
Bacterial, viral, fungal, and parasitic pathogens can trigger meningeal inflammation. Noninfectious meningitis pathways can also occur in select medication-triggered or autoimmune contexts. Because the inflammatory process occurs near central nervous system tissue, edema and rising ICP can develop quickly and cause severe neurologic compromise.
Classification
- Bacterial meningitis: High-acuity infection with rapid deterioration risk and urgent broad-spectrum anti-infective treatment.
- Viral meningitis: Often less severe, with neurologic effects that are commonly temporary and recovery after inflammation resolves.
- Meningococcal meningitis: Highly contagious bacterial form requiring immediate emergency response and public health precautions.
Risk Factors
- Higher nasopharyngeal colonization risk in children and adolescents.
- Recent respiratory or ENT infection (for example otitis media, sinus disease, mastoiditis, or dental abscess) that can seed meningeal spaces.
- Immunosuppression (for example chemotherapy, chronic steroid exposure, immunosuppressive therapy, or HIV context).
- Neonatal exposure risk from maternal Group B streptococcus colonization/infection.
- Dense communal-living settings (for example campus or military housing) in meningococcal spread scenarios.
- Male sex and close-quarter living settings in outbreak-prone populations.
- Skull-fracture or neurosurgical-barrier disruption increasing pathogen entry risk.
- Travel to higher-prevalence regions in selected outbreak contexts.
Nursing Assessment
NCLEX Focus
Prioritize early recognition of neurologic decline and ICP-related findings while initiating isolation and escalation.
- Assess for classic findings: severe headache, neck rigidity, high fever, acute confusion, photophobia, phonophobia, nausea or vomiting, and petechiae.
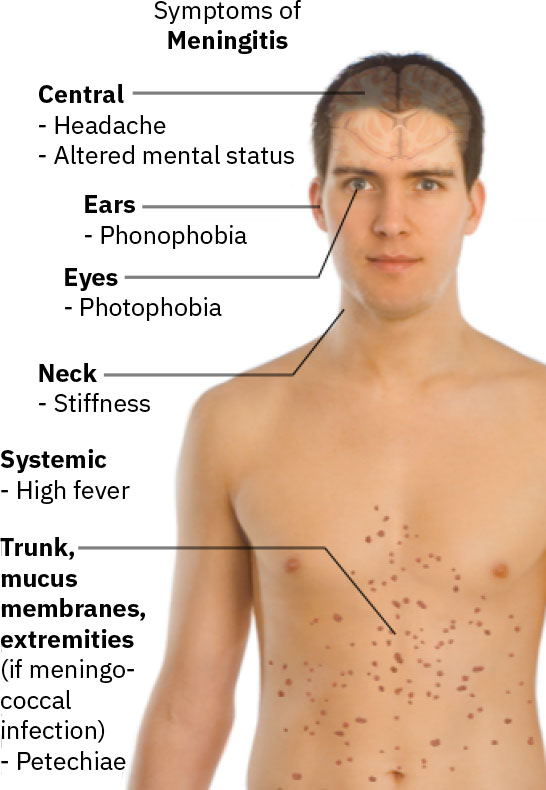 Illustration reference: OpenStax Medical-Surgical Nursing Ch.17.2.
Illustration reference: OpenStax Medical-Surgical Nursing Ch.17.2.
- Assess the classic triad pattern (neck stiffness, fever, altered mental status), while recognizing some clients present with incomplete triad findings.
- In suspected meningococcal disease, assess for lower-extremity petechial rash and rapid sepsis progression cues (tachycardia, tachypnea, hypotension).
- Assess for meningeal signs, including Brudzinski and Kernig findings, while recognizing they appear in only a minority of clients.
- Kernig sign: pain/resistance with attempted knee extension from flexed hip-knee position; Brudzinski sign: involuntary hip-knee flexion with passive neck flexion.
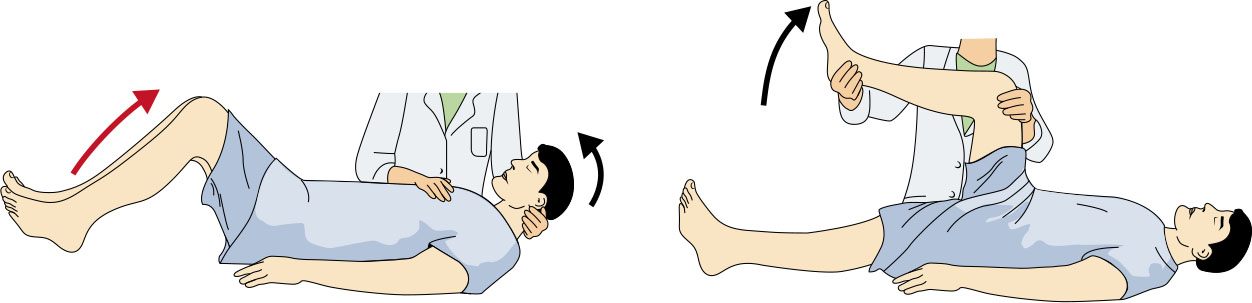 Illustration reference: OpenStax Medical-Surgical Nursing Ch.17.2.
Illustration reference: OpenStax Medical-Surgical Nursing Ch.17.2.
- Monitor for seizure activity, altered level of consciousness, focal deficits, and signs of worsening cerebral perfusion.
- In infants, assess nonspecific deterioration cues such as fatigue, irritability, and distended fontanelle.
- Trend vital patterns suggestive of ICP concerns, including rising blood pressure with relative bradycardia.
- Recognize that high fever may be absent in older adults or immunosuppressed clients, including those already on antibiotics.
- Review diagnostics: CSF analysis from lumbar puncture (opening pressure, WBC, protein, glucose), blood cultures, CBC, electrolytes, liver enzymes, and targeted infectious studies (including HIV testing when indicated).
- Review additional workup cues when associated infections are suspected (for example throat/nasal/urine cultures and chest/sinus/mastoid imaging).
- Use CT before lumbar puncture in high-herniation-risk clients (for example age >60 years, immunosuppression, or signs of elevated ICP).
Nursing Interventions
- Administer prescribed broad-spectrum IV antibiotics immediately, then support transition to organism-specific therapy after culture and Gram stain results.
- In suspected meningococcal meningitis, do not delay empiric antibiotics while awaiting confirmatory laboratory results.
- Prepare for prolonged IV antibacterial therapy courses (often 2-3 weeks) in bacterial disease contexts.
- Administer adjunct medications as ordered, such as dexamethasone, seizure therapy, and ICP-directed therapy; corticosteroid use may vary by protocol and clinical context.
- Provide symptom-relief support (for example ordered analgesic/antipyretic pathways) for fever, pain, and discomfort.
- Perform frequent neurologic assessments and document trends to detect early deterioration.
- Reduce environmental stimulation and position head of bed 30-45 degrees with midline head alignment to support ICP management.
- Implement droplet precautions for bacterial meningitis and reinforce exposure management for close contacts.
- Support fluid and electrolyte balance with ordered IV hydration and targeted electrolyte correction when needed.
- Support oxygenation and ventilation when respiratory effort declines or neurologic burden worsens.
- Assist with ordered drainage procedures (for example mastoid or sinus drainage) in selected bacterial disease pathways.
- Monitor for SIADH-associated hyponatremia and worsening ICP risk when ADH dysregulation is suspected.
Time-Critical Neurologic Deterioration
Untreated or progressing meningitis can rapidly lead to increased ICP, herniation, and death.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| antibiotics (broad-spectrum-antibiotics) | empiric IV therapy, then targeted agents | Start promptly; adjust after culture and susceptibility data return. |
| corticosteroids | dexamethasone | Used in community-acquired bacterial meningitis to reduce complications. |
| diuretics (osmotic-diuretics) | mannitol | Supports ICP reduction when cerebral edema risk is present. |
| anticonvulsants | class-based agents | Used when seizure activity occurs or risk escalates. |
| antibiotics (prophylactic-antibiotics) | rifampicin, ciprofloxacin, ceftriaxone | Given to close contacts in meningococcal exposure scenarios. |
Health Teaching
- Teach effective hand hygiene and respiratory etiquette to reduce transmission risk during illness episodes.
- Teach vaccine-based prevention of bacterial meningitis, including meningococcal, pneumococcal, and Hib vaccine pathways.
- Reinforce keeping age-appropriate immunization schedules current for adults and children.
- In meningococcal exposure settings, teach close-contact prophylaxis adherence and urgent symptom reporting.
- In pediatric hospitalization, encourage caregiver participation in care to reduce anxiety and support orientation.
- Teach that post-discharge hearing screening is recommended around 4 weeks after meningitis recovery to detect delayed hearing loss.
Clinical Judgment Application
Clinical Scenario
A young adult living in group housing presents with abrupt fever, severe headache, neck stiffness, photophobia, and confusion, with worsening neurologic responsiveness over several hours.
- Recognize Cues: Acute meningeal symptoms with mental-status change and rapid progression.
- Analyze Cues: Findings are consistent with high-risk bacterial meningitis and rising ICP risk.
- Prioritize Hypotheses: Immediate priority is preventing neurologic decompensation and death.
- Generate Solutions: Begin emergency anti-infective pathway, isolation, and serial neurologic monitoring.
- Take Action: Administer ordered therapy without delay, implement droplet precautions, and escalate changes rapidly.
- Evaluate Outcomes: Stabilized neurologic exam, controlled temperature, and no further ICP progression.
Related Concepts
- common-neurological-disorders-recognition-and-priority-care - Differential neurologic assessment framework for acute deterioration.
- intracranial-hypertension-and-increased-intracranial-pressure - Cross-etiology ICP recognition, diagnostics, and stabilization priorities.
- ear-assessment-hearing-tests-and-common-abnormalities - Postmeningitis hearing surveillance and referral context.
- anaphylaxis - Critical emergency comparison for rapid airway and circulation prioritization.
- medication-administration-safety-measures - High-risk IV medication safety and reassessment during urgent therapy.
- sodium-balance-disorders - Potential ADH-related sodium disturbance that can worsen neurologic risk.
- systematic-ecg-interpretation-and-dysrhythmia-triage - Cardiac monitoring relevance during severe neurologic and electrolyte instability.
Self-Check
- Which findings most strongly suggest high-risk bacterial meningitis rather than mild viral illness?
- Why are early antibiotics and neurologic trend monitoring both time-critical in meningitis care?
- Which assessment changes indicate escalating ICP and immediate intervention needs?