Intracranial Hypertension and Increased Intracranial Pressure
Key Points
- Adult intracranial pressure is commonly about 7-15 mm Hg, with broader critical-care references often citing about 1-20 mm Hg; sustained pressure above about 20-25 mm Hg generally triggers treatment escalation.
- The skull is a fixed-volume compartment; increases in brain tissue, blood, CSF, or added pathologic mass can raise intracranial pressure.
- Intracranial hypertension can progress to symptomatic increased ICP with neurologic deterioration.
- High-risk progression includes cerebral edema, seizures, and brain herniation.
- Cushing triad (widened pulse pressure, bradycardia, irregular respirations) is a late, high-acuity deterioration cue.
- Priority bedside actions include rapid recognition, head-of-bed elevation (about 30 degrees), neutral neck alignment, and urgent escalation.
Pathophysiology
Intracranial pressure dynamics follow the Monro-Kellie doctrine (fixed-volume principle): the adult cranial vault is mostly brain tissue with smaller blood and cerebrospinal fluid (CSF) fractions. Compensation occurs by shifting CSF and blood volume, but once reserve is exceeded, pressure rises rapidly.
Intracranial hypertension refers to elevated pressure within the skull, while increased intracranial pressure describes a pressure rise associated with clinical deterioration risk. Common drivers include trauma, hemorrhage, tumors or mass lesions, infection, and edema.
Classification
- Intracranial hypertension: Elevated intracranial pressure that may initially have limited symptoms.
- Increased intracranial pressure (ICP): Pressure elevation with clinical manifestations such as headache, nausea/vomiting, visual change, altered mental status, and vital-sign changes.
Nursing Assessment
NCLEX Focus
Trend neurologic status and deterioration cues continuously; delayed escalation increases herniation risk.
- Assess for headache, nausea/vomiting, blurred vision, dizziness, tinnitus, confusion, and level-of-consciousness decline.
- Treat subtle baseline-to-trend LOC change (for example new drowsiness or mild confusion) as an early high-priority cue.
- Assess for severe-progression cues: seizures, papilledema, bradycardia with hypertension pattern, pupillary change, respiratory-pattern changes, and coma progression.
- Include sudden projectile-vomiting pattern, even without preceding nausea, as a potential increased-ICP deterioration finding.
- Assess for pathologic motor posturing (decorticate, decerebrate, or flaccid) as high-risk neurologic deterioration signs.
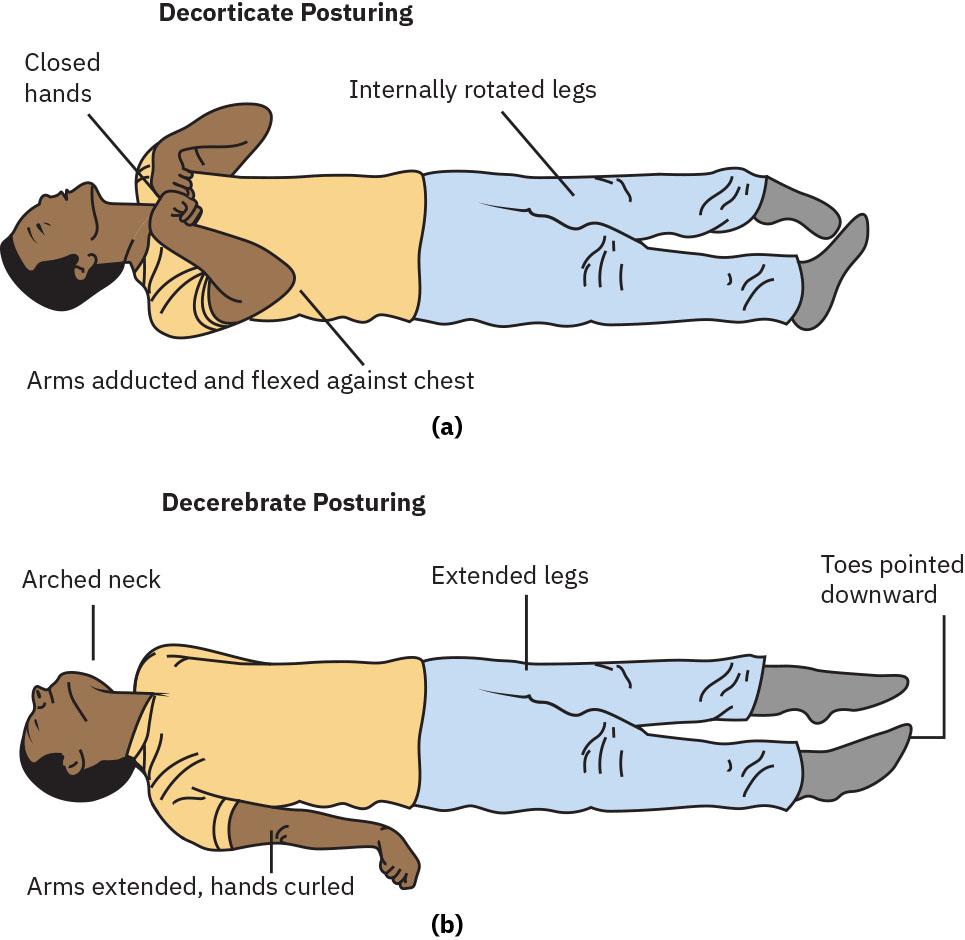 Illustration reference: OpenStax Medical-Surgical Nursing Ch.35.4.
Illustration reference: OpenStax Medical-Surgical Nursing Ch.35.4.
- Assess for suspected brain-herniation cues (for example unilateral/bilateral pupil dilation and loss of consciousness) and escalate emergently.
- Use Glasgow Coma Scale trend as a severity marker; scores below 8 indicate high-risk deterioration requiring intensive monitoring/escalation.
- Review etiology context: trauma, bleeding, infection, tumor/mass, or other neurologic injury drivers.
- Use diagnostics to confirm severity and cause: CT/MRI, focused neurologic assessment, and direct ICP monitoring when indicated.
- Include targeted vascular and CSF diagnostics when ordered (for example cerebral angiography and CSF analysis) to clarify cause.
- Recognize direct intracranial pressure catheter measurement as the gold-standard diagnostic and monitoring method in critical pathways.
- Distinguish ICP-monitoring device roles: intraventricular catheters allow direct pressure measurement plus CSF drainage, while parenchymal monitors provide tissue-pressure trend data.
- Include transcranial Doppler and ophthalmologic optic-nerve assessment when ordered to support noninvasive trend interpretation.
Nursing Interventions
- Escalate early for worsening neurologic exam, seizure activity, papilledema cues, or suspected herniation.
- Keep head of bed at about 30 degrees (or ordered angle) and maintain neutral neck alignment to support venous drainage and ICP control.
- Reduce Valsalva-provoking triggers (for example straining, forceful coughing, or bearing down) using bowel-regimen and airway support strategies as ordered.
- Implement fever prevention and treatment measures because hyperthermia can worsen ICP burden.
- Use pharmacologic and nonpharmacologic pain-control measures because pain and stress can increase ICP.
- Support oxygenation and ventilator-management adjustments when ordered to maintain brain oxygen delivery and reduce secondary ICP worsening.
- Track MAP and cerebral perfusion targets; many ICU pathways maintain MAP around 70-90 mm Hg to support adequate cerebral perfusion pressure.
- Support airway/oxygenation and continuous neurologic reassessment in high-risk deterioration states.
- Administer ordered ICP-directed therapy and monitor response with serial neuro checks, vital signs, fluid balance, and laboratory trends.
- Support invasive ICP pathways when ordered (for example ventriculostomy with external ventricular drainage for pressure monitoring and CSF diversion).
- Apply seizure precautions in moderate-to-severe deterioration pathways because worsening ICP can precipitate seizure activity.
- Reinforce post-craniectomy protection precautions (for example ordered helmet use during mobility) in decompressive-surgery recovery pathways.
- Monitor for treatment complications such as electrolyte shifts, metabolic acidosis, dehydration, renal injury, or pulmonary edema.
Herniation Risk
Progressive ICP elevation can rapidly cause irreversible brain injury, respiratory failure, and death.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| Carbonic anhydrase inhibitors | Acetazolamide | Lowers CSF production and can reduce ICP; monitor sodium/potassium and acid-base status; avoid in significant hepatic disease and major electrolyte imbalance. |
| Hyperosmolar therapy | Mannitol, hypertonic saline | Pulls water from brain tissue to reduce edema and ICP; monitor serum osmolality, urine output, renal function, and volume-overload or pulmonary-edema cues. Avoid rapid infusion that can worsen fluid shifts and rebound cerebral edema. |
| Adjunct neurologic stabilization regimens | Barbiturate/sedative/antiepileptic pathways | Used in selected severe cases; monitor respiratory status, hemodynamics, and neurologic response continuously. |
Clinical Judgment Application
Clinical Scenario
A hospitalized client with acute neurologic injury develops worsening headache, new confusion, bradycardia, and unequal pupils.
- Recognize Cues: Rapid neurologic deterioration with ICP-compromise pattern.
- Analyze Cues: Increased intracranial pressure with possible impending herniation is likely.
- Prioritize Hypotheses: Prevent irreversible brain injury by immediate ICP-directed stabilization.
- Generate Solutions: Elevate head of bed, maintain neutral neck alignment, activate emergency escalation, and prepare ordered hyperosmolar therapy.
- Take Action: Implement rapid neuro-monitoring workflow and administer treatment per protocol/provider orders.
- Evaluate Outcomes: Neurologic status and vital signs stabilize with reduced deterioration cues.
Related Concepts
- meningitis-priority-care-and-icp-risk - Infectious neurologic pathway with ICP escalation overlap.
- traumatic-brain-injury - Trauma-associated secondary swelling and pressure deterioration.
- stroke - Hemorrhagic or large-ischemic injury can precipitate elevated ICP.
- diuretics - Osmotic and CAI pathways used in selected ICP management plans.
- neurological-diagnostic-testing-and-nursing-considerations - ICP monitoring and imaging safety workflow.
- anticonvulsants - Seizure-control support in high-risk intracranial emergencies.
- intracranial-hypotension-and-decreased-intracranial-pressure - Lower-pressure intracranial state requiring opposite positioning strategy.
Self-Check
- Which bedside findings suggest progression from intracranial hypertension to life-threatening increased ICP?
- Why are head-of-bed elevation and neutral neck positioning standard early ICP-support interventions?
- What monitoring data are priority during mannitol or acetazolamide therapy?