Ear Assessment Hearing Tests and Common Abnormalities
Key Points
- Ear assessment includes symptom interview, structural inspection/palpation, otoscopic findings, and focused hearing tests.
- Weber and Rinne tuning-fork tests help separate conductive from sensorineural loss patterns.
- Severe pain, mastoid tenderness, sudden hearing loss, vertigo with neurologic signs, or traumatic injury findings require urgent escalation.
- Functional interpretation requires linking outer-, middle-, and inner-ear findings with both hearing and equilibrium symptoms.
Pathophysiology
Hearing and balance depend on integrated external, middle, and inner ear function. Mechanical transmission defects cause conductive loss, while cochlear, vestibular, or neural injury causes sensorineural deficits.
Because vestibular and auditory systems are linked, ear pathology can present as hearing change, tinnitus, disequilibrium, or falls. The outer ear (pinna and canal) collects/directs sound, the middle ear (tympanic membrane, ossicles, eustachian tube) transmits and amplifies vibration while pressure-balancing, and the inner ear (cochlea plus vestibular apparatus) converts mechanical signals to neural input for hearing and balance.
Pediatric ear anatomy changes risk distribution: children have smaller, more horizontally oriented eustachian tubes, which can reduce drainage efficiency and increase otitis risk.
Classification
- Assessment domains: External ear/canal findings, tympanic membrane cues, hearing pattern and balance symptoms.
- Anatomy-function domains: Outer-ear collection, middle-ear amplification/pressure equalization, and inner-ear auditory-vestibular transduction.
- Loss-pattern class: Conductive, sensorineural, or mixed hearing impairment.
- Conductive-loss examples: Cerumen impaction, tympanic-membrane perforation, and other external/middle-ear obstruction patterns.
- Sensorineural-loss examples: Inner-ear/cochlear injury, CN VIII pathology, age-related presbycusis, and ototoxic-medication exposure.
- Age-related pattern: Presbycusis (usually gradual, bilateral, and most apparent in speech-in-noise settings).
- Abnormality groups: Inflammatory/infectious, obstructive, congenital/structural, and trauma-related conditions.
- External-structure abnormality examples: Microtia, macrotia, Stahl-ear morphology variants, congenital tags/pits, and trauma-related cauliflower-ear deformity.
- Tympanic-membrane abnormality examples: Perforation, tympanosclerosis/scarring, retraction, myringitis, and acute/chronic otitis-media-associated changes.
- Inner-ear abnormality examples: Meniere-pattern episodic vertigo with fluctuating hearing/tinnitus/fullness, labyrinthitis, and trauma-related cochlear-vestibular injury.
Nursing Assessment
NCLEX Focus
Prioritize sudden hearing change, vestibular instability, and infection-spread cues before routine chronic findings.
- Assess ear pain, discharge, hearing change, tinnitus, vertigo, and prior trauma/water exposure.
- Obtain focused history for onset/progression, infection/discharge history, prior procedures, ototoxic/other medication exposure, and functional impact on communication/work/safety.
- Assess for reversible contributors (for example cerumen impaction) and long-term noise exposure history.
- Assess personal ear-care habits (for example cotton-swab or foreign-object insertion) that may cause canal trauma or obstruction.
- Assess social-withdrawal or “smiling/nodding without congruent answers” patterns that may indicate unreported hearing difficulty rather than cognitive decline alone.
- Inspect and palpate auricle, canal entrance, and mastoid area for tenderness, edema, and erythema.
- In external-canal infection concern, assess for erythematous/edematous canal, debris, pruritus, and pain worsened by upward-outward auricle traction; use otitis-externa cues to screen for malignant-progression risk in high-risk clients.
- Assess for cerumen impaction or foreign body as reversible obstructive causes of pain, hearing decline, and incomplete tympanic visualization.
- Use otoscopic exam to assess canal skin/obstruction and tympanic-membrane color, position, integrity, and landmarks; note bulging, retraction, perforation, or fluid.
- Correlate tympanic findings with pressure/infection history (for example recurrent otitis-media, post-URI ear pain/irritability, or tube-placement history).
- In pediatric acute ear-pain presentations, assess for bulging erythematous tympanic membrane findings and re-evaluate pain response after initial analgesic intervention.
- Use structured hearing checks, including tuning-fork comparisons when indicated.
- During conversational screening, suspect hearing impairment when the patient persistently lip-reads, strains to hear, requests repetition frequently, or uses inappropriately loud speech.
- For whispered-voice screening, test each ear separately with contralateral occlusion while standing behind the patient at about arm’s length to reduce lip-reading bias.
- Use low-volume mixed letter-number sequences (for example 4-K-2), repeating with a different sequence if first response is incorrect.
- Treat correct repetition of at least 3 out of 6 whispered items per ear as a practical bedside pass threshold.
- Interpret tuning-fork findings explicitly: Weber lateralization can indicate asymmetry; Rinne positive (AC > BC) suggests normal/sensorineural pattern, while Rinne negative (BC >= AC) supports conductive loss in that ear.
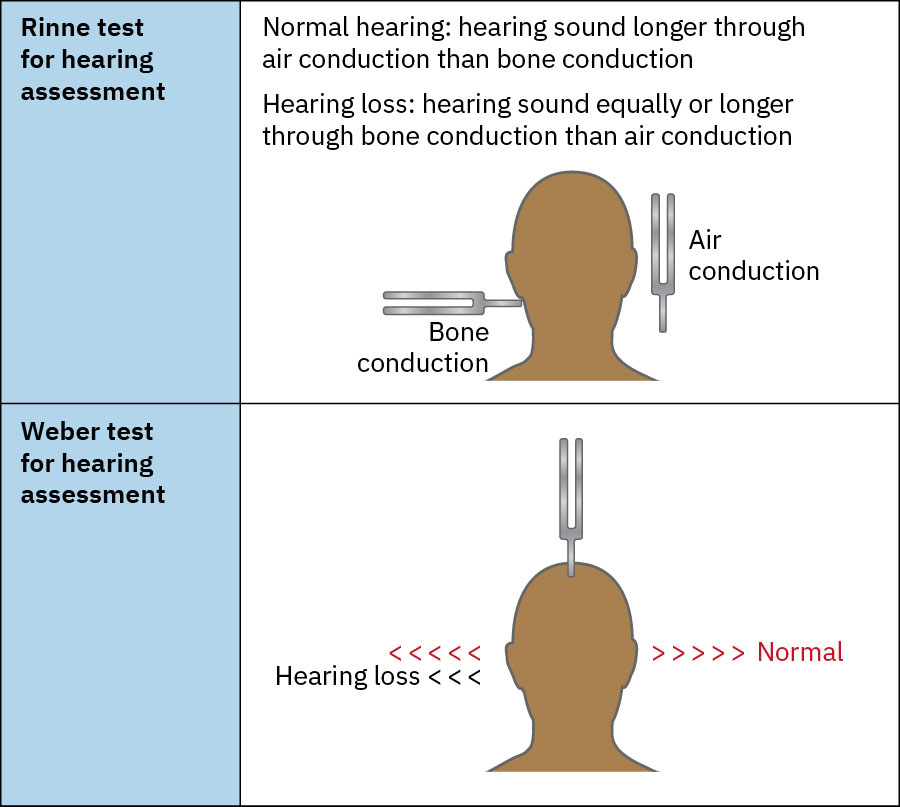 Illustration reference: OpenStax Clinical Nursing Skills Ch.22.3.
Illustration reference: OpenStax Clinical Nursing Skills Ch.22.3.
- Apply age-appropriate otoscopic technique (positioning/cooperation strategy and speculum size) to reduce discomfort and improve exam quality in infants/young children.
- For younger children, straighten the canal by pulling the auricle down and back; in older children, pull up and back to optimize tympanic-membrane visualization.
- Assess equilibrium with gait/posture observation and Romberg comparison (eyes open then eyes closed) while guarding for fall risk.
- If Romberg worsens only after eye closure, consider proprioceptive/vestibular dysfunction; instability in both conditions suggests broader balance impairment.
- Screen for tinnitus and vertigo pattern detail (onset, triggers, nausea/vomiting, functional impact) and correlate with hearing-change findings.
- In episodic vertigo with fluctuating hearing, tinnitus, and aural fullness, escalate inner-ear disorder evaluation.
- In positional “room spinning” vertigo presentations, assess for benign paroxysmal positional vertigo (BPPV) pattern and related fall-risk impact.
- Include facial-nerve (CN VII) asymmetry screening when ear/vestibular complaints coexist.
- Document hearing pattern changes and associated safety impacts (communication breakdown, falls, disorientation).
Nursing Interventions
- Escalate red flags such as sudden unilateral hearing loss, severe vertigo, mastoid pain, or trauma-associated deficits.
- Implement communication adaptation and fall-risk precautions when hearing or balance is compromised.
- Reinforce hearing-protection practices for ongoing occupational/recreational noise exposure.
- Teach safe ear-care behaviors (avoid inserting objects into the ear canal unless specifically directed).
- Reinforce safe ear-care practices and medication adherence for treated conditions.
- For otitis-externa treatment plans, reinforce correct otic-drop administration, pain-trend reassessment, and urgent return precautions for fever or poor response.
- Support cerumen-management pathway when indicated (softening drops, irrigation, or manual removal per protocol) and reassess hearing plus tympanic findings after clearance.
- For BPPV-pattern findings, support referral to trained clinicians for canalith-repositioning maneuvers and reinforce safety precautions until symptoms stabilize.
- Escalate failed bedside hearing screening (for example inability to repeat whispered words) for audiology referral and follow-up planning.
- Validate uncertain findings through repeat exam, equipment checks, patient confirmation, and second-clinician verification when needed.
- Document otoscopic detail consistently (canal findings, cerumen/discharge, tympanic landmarks, bulging/retraction/perforation, balance findings, and hearing-test results).
Rapid Deterioration Risk
Missed sudden hearing or vestibular changes can delay treatment and increase fall and injury risk.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| ototoxic-medications | Selected loop-diuretics (loop diuretics) and others | Monitor new hearing/tinnitus/vertigo trends and escalate early. |
| Otic Antibiotics | Topical antibiotic drops | Ensure correct administration technique and reassess symptom progression. |
Clinical Judgment Application
Clinical Scenario
A patient with new ear pain reports muffled hearing and dizziness; mastoid palpation is tender.
- Recognize Cues: Combined hearing and balance change with posterior-ear tenderness.
- Analyze Cues: Pattern suggests more than simple transient obstruction.
- Prioritize Hypotheses: Immediate priority is preventing progression and injury from instability.
- Generate Solutions: Initiate escalation pathway and implement safety precautions.
- Take Action: Notify provider, document objective findings, and support safe mobility/communication.
- Evaluate Outcomes: Early intervention reduces complication and fall risk.
Related Concepts
- assisting-with-sensory-deficits - Hearing-support strategies reduce communication and safety failures.
- medication-effects-on-sensory-perception-and-safety - Explains medication-linked hearing and vestibular changes.
- fall-prevention - Vestibular symptoms directly increase fall risk.
- otitis-externa - External-canal infection management and malignant-risk escalation context.
- otitis-media - Middle-ear infection versus effusion differentiation and hearing-language risk management.
- documenting-and-reporting-data - Structured reporting improves continuity and escalation quality.
Self-Check
- How do Weber and Rinne findings support differentiation of hearing-loss patterns?
- Which ear findings should trigger urgent rather than routine follow-up?
- Why are mobility precautions critical when vestibular symptoms are present?