Thyroid Disorders
Key Points
- Hypothyroidism and hyperthyroidism produce opposite metabolic patterns but both can destabilize cardiovascular and neurologic function if untreated.
- Priority assessment differentiates low-metabolic versus high-metabolic symptom clusters, then confirms with thyroid laboratory trends.
- Graves disease is the most common cause of hyperthyroidism and can include exophthalmos and goiter.
- Core diagnostics include TSH with free T4 and selected adjunct tests based on suspected cause and severity.
- Nursing management combines medication safety, symptom surveillance, and escalation for thyroid storm or myxedema-risk deterioration.
- Simple goiter reflects thyroid enlargement, commonly from iodine deficiency with compensatory TSH-driven gland growth.
- Iodine imbalance can worsen thyroid dysfunction in both directions, so bedside screening of salt source and diet pattern is high-yield.
Pathophysiology
Thyroid disorders reflect dysregulation of the hypothalamic-pituitary-thyroid axis and altered circulating thyroid hormone effect at tissue level. In hypothyroidism, reduced thyroid-hormone activity slows metabolic processes and can lead to fatigue, cold intolerance, weight gain, slowed cognition, and cardiovascular decompensation if severe.
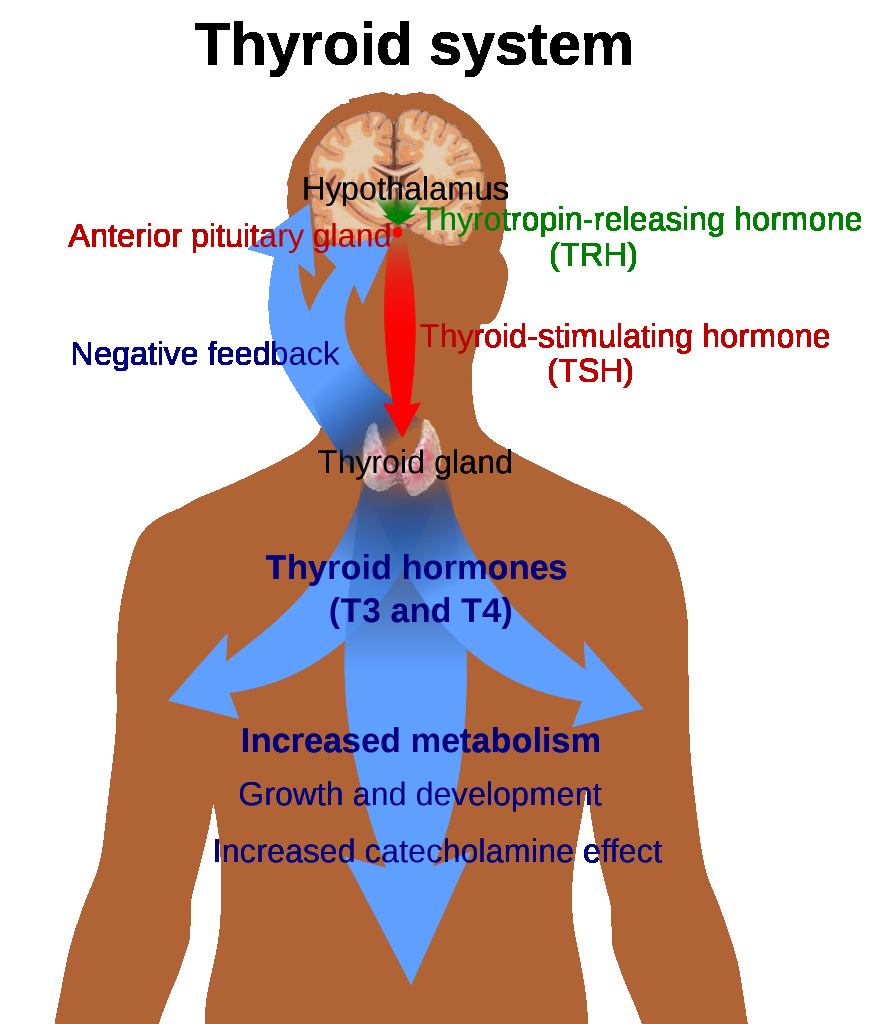 Illustration reference: OpenRN Health Alterations Ch.7.2.
Illustration reference: OpenRN Health Alterations Ch.7.2.
In hyperthyroidism, excessive thyroid-hormone effect increases metabolic demand and sympathetic-like manifestations, including heat intolerance, weight loss, tremor, anxiety, and tachyarrhythmia risk. Graves-pattern hyperfunction is a common primary etiology. Some hyperthyroid presentations are phenotype-specific, including T3 toxicosis (high T3 with low TSH and normal T4) and subclinical hyperthyroidism (low TSH with normal T3/T4). When iodine intake is insufficient, thyroid hormone synthesis falls and compensatory TRH-TSH drive persists, causing follicular colloid accumulation and thyroid enlargement (goiter). In iodine-replete settings, goiter is often autoimmune in origin, and excessive iodine intake can aggravate hyperthyroid-pattern instability in susceptible patients. Selenium status can also influence thyroid-hormone metabolism; combined iodine and selenium inadequacy may worsen thyroid dysfunction risk.
Classification
- Hypothyroid pattern: Low thyroid-hormone effect with reduced metabolic activity.
- Hyperthyroid pattern: Excess thyroid-hormone effect with accelerated metabolic activity.
- Acute high-risk state: Thyroid storm spectrum requiring immediate escalation.
- Acute low-metabolic decompensation risk: Severe hypothyroid deterioration requiring urgent evaluation and supportive stabilization.
- Simple goiter (endemic goiter): Noncancerous thyroid enlargement often linked to inadequate iodine intake.
- Iodine-deficiency burden pattern: Prolonged deficiency can impair fertility, fetal-infant outcomes, and neurodevelopment.
- Congenital hypothyroidism pattern: Untreated thyroid-hormone deficiency in early life can cause major neurodevelopmental and growth deficits.
Nursing Assessment
NCLEX Focus
Prioritize recognition of opposite symptom clusters and identify which findings require immediate provider escalation.
- Compare symptom direction: weight gain/cold intolerance/fatigue versus weight loss/heat intolerance/tremor/palpitations.
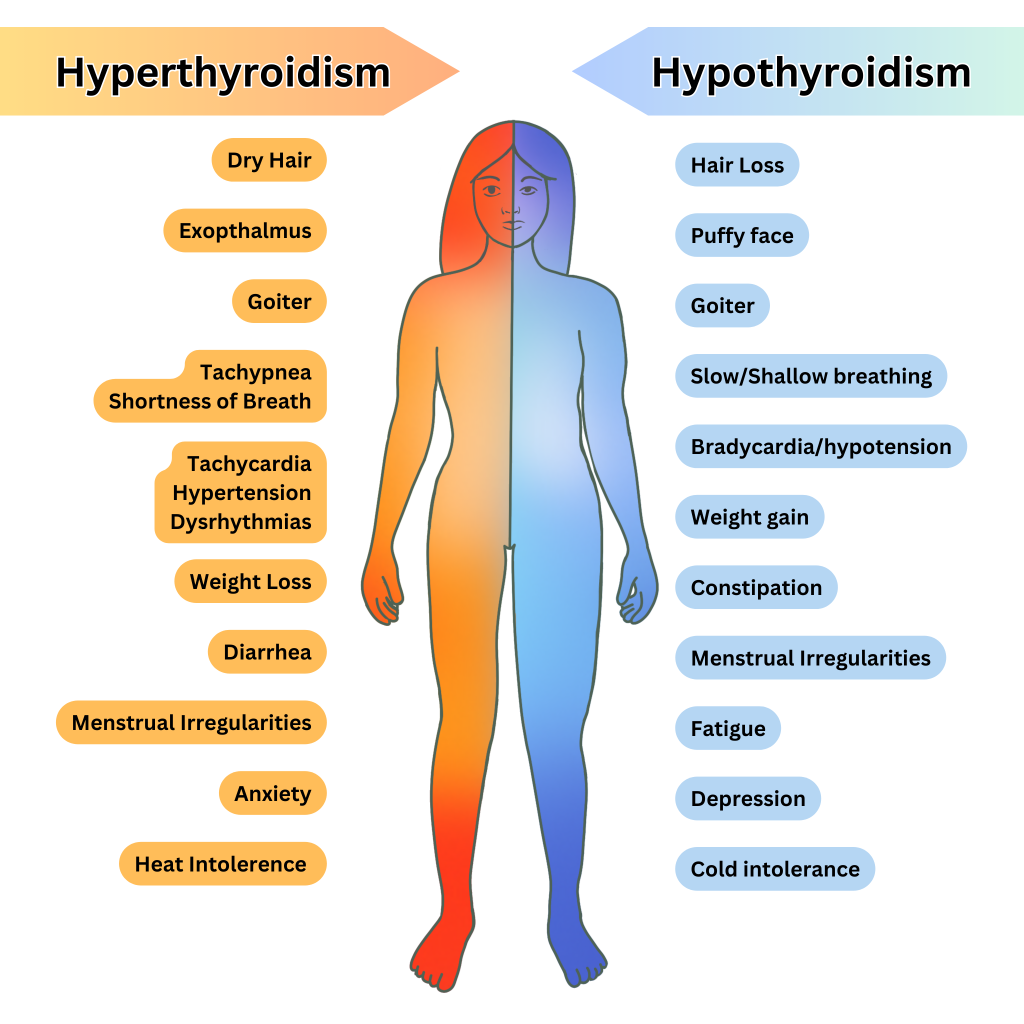 Illustration reference: OpenRN Health Alterations Ch.7.6.
Illustration reference: OpenRN Health Alterations Ch.7.6.
- In severe hypothyroid patterns, assess myxedema-associated tissue changes such as facial/periorbital puffiness, thickened dry-waxy skin, brittle hair or nails, and hoarseness.
- Monitor cardiovascular signs closely, especially tachycardia, rhythm change, blood-pressure instability, and activity intolerance.
- Trend thyroid diagnostics (TSH and free T4) with symptom progression rather than isolated values.
- Assess for enlargement or structural thyroid findings and correlate with swallowing, airway, or neck discomfort complaints.
- Assess visible anterior-neck enlargement patterns consistent with goiter and correlate with iodine-intake history and thyroid-lab trends.
- Ask specifically about iodine exposure pattern, including iodized versus non-iodized salt use and low-iodine diet patterns (for example very limited seafood, dairy, and egg intake).
- In hyperthyroid-pattern assessment, screen for exophthalmos, fine tremor, diaphoresis, and thyroid bruit findings when gland hypervascularity is suspected.
- In postpartum clients, screen for transient postpartum thyroiditis (fatigue, heat/cold intolerance, palpitations, and mood/cognitive changes) during the first year after delivery.
- Escalate suspicious thyroid nodules for targeted imaging and fine-needle-biopsy evaluation when malignancy concern is present.
- Screen goiter-associated compressive symptoms (for example dysphagia or dyspnea) and escalate progressive airway/swallow compromise.
- Screen hyperthyroid-predominant bowel and rhythm cues (for example diarrhea and irregular tachyarrhythmia) and hypothyroid-predominant cues (for example constipation and bradycardia).
- Screen for acute deterioration cues: severe hypermetabolic instability or severe mental-status and perfusion decline in hypothyroid presentations.
- Recognize thyroid-storm red flags, including high fever (often above 105 F), agitation or confusion, restlessness, and severe cardiovascular instability.
- Recognize myxedema-coma risk cues, including hypothermia, bradycardia, hypotension, hypoventilation, and declining mental status.
Nursing Interventions
- Reinforce medication adherence timing and monitoring plan for both thyroid replacement and antithyroid therapy.
- Reinforce follow-up laboratory cadence after therapy changes (commonly every 4-8 weeks during titration, then longer maintenance intervals once stable).
- Coordinate laboratory follow-up and symptom reassessment after treatment adjustments.
- Teach patients to report worsening palpitations, chest pain, dyspnea, confusion, persistent fever, or marked functional decline immediately.
- Support rest-energy balance, temperature comfort strategies, and safe activity pacing during treatment titration.
- Use interprofessional referral pathways when endocrine instability affects cardiac safety, nutrition, or psychosocial coping.
- Escalate suspected myxedema-coma risk promptly and prepare for airway, hemodynamic, and temperature-support interventions.
- In myxedema-coma pathways, anticipate ICU-level care with continuous cardiac monitoring and IV thyroid-hormone replacement.
- Reinforce iodine-adequate nutrition guidance when deficiency-related goiter is suspected and coordinate follow-up for persistent neck enlargement.
- Teach that deficiency-related simple-goiter enlargement may improve with consistent iodine repletion and ongoing thyroid monitoring.
- For Graves or other hyperthyroid-pattern clients, avoid excess iodine supplementation and coordinate individualized intake guidance with endocrine and nutrition teams.
- For hyperthyroid symptom burden, support high-calorie nutrition, ocular-surface protection (lubrication), and rhythm/temperature monitoring.
- In thyroid-storm risk windows, monitor for hyperthermia, tachycardia, hypertension, and neurologic decline; escalate urgently for ICU-directed therapy.
Thyroid Emergency Escalation
Rapid decompensation with severe hypermetabolic instability or severe hypothyroid decline is a high-risk state and requires immediate emergency-provider escalation.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| thyroid-medications | levothyroxine, liothyronine | Thyroid hormone replacement requires trend-based titration with follow-up TSH monitoring. |
| thyroid-medications | methimazole, propylthiouracil | Antithyroid-agent safety includes CBC trend monitoring and urgent fever or sore-throat reporting. |
| beta-blockers | class-based adjuncts | Used for tremor/tachycardia symptom control while thyroid levels are corrected. |
Clinical Judgment Application
Clinical Scenario
An adult with known thyroid disease reports progressive palpitations, heat intolerance, and unintended weight loss with worsening anxiety and insomnia.
- Recognize Cues: Hypermetabolic symptom cluster with cardiovascular risk signs.
- Analyze Cues: Possible uncontrolled hyperthyroid state with escalation risk.
- Prioritize Hypotheses: Immediate safety concern is progression toward unstable endocrine-cardiac status.
- Generate Solutions: Urgent reassessment, lab review, medication-plan confirmation, and rapid provider escalation.
- Take Action: Initiate escalation workflow and continuous symptom-safety monitoring.
- Evaluate Outcomes: Symptoms stabilize and treatment plan is adjusted with clear follow-up thresholds.
Related Concepts
- endocrine-system - Core hormone-axis physiology supporting thyroid interpretation.
- thyroid-medications - Medication classes used for hypo- and hyperthyroid treatment.
- systematic-ecg-interpretation-and-dysrhythmia-triage - Hyperthyroid states increase arrhythmia risk.
- leukopenia-and-neutropenia - Antithyroid therapy adverse-effect surveillance overlaps with neutropenia risk cues.
- adult-preventive-screening-and-health-promotion - Ongoing follow-up and symptom education reduce delayed complication risk.
Self-Check
- Which symptom pattern most strongly distinguishes hypothyroidism from hyperthyroidism at initial triage?
- Why are serial thyroid laboratory trends more useful than a single isolated value?
- Which signs require immediate escalation for potential thyroid-related decompensation?