Alcohol Use Disorder
Key Points
- AUD is a chronic brain disorder marked by impaired control of alcohol use despite social, medical, and occupational harm.
- Heavy drinking thresholds are at least 8 drinks/week for women and 15 drinks/week for men; binge drinking is at least 4 drinks for women or 5 drinks for men per occasion.
- A standard drink contains 14 g (0.6 oz) of pure alcohol.
- Moderation guidance is up to 1 drink/day for women and up to 2 drinks/day for men.
- Binge drinking (4 or more drinks for women or 5 or more drinks for men in about 2 hours) can raise BAC to 0.08% or higher and increase injury risk.
- Withdrawal can progress to seizures or delirium-tremens, requiring rapid protocol-based management.
- Alcohol overdose can suppress breathing and protective airway reflexes; emergency positioning and airway protection reduce aspiration-related death risk.
- Disulfiram deters relapse by causing an aversive acetaldehyde reaction with alcohol; start only after recent abstinence and continue alcohol avoidance after stopping the drug.
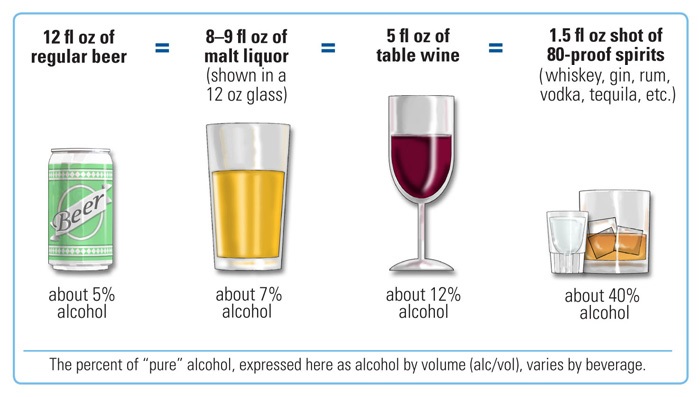 Illustration reference: OpenRN Nursing Health Promotion Ch.6.5.
Illustration reference: OpenRN Nursing Health Promotion Ch.6.5.
Pathophysiology
Alcohol dysregulates inhibitory and excitatory neurotransmission and reinforces reward circuitry. Repeated exposure produces tolerance and dependence, then withdrawal hyperexcitability when intake abruptly decreases. This physiologic instability underlies tremor, autonomic overactivity, anxiety, and severe complications.
AUD severity is classified as mild, moderate, or severe based on diagnostic burden and functional impact. Co-occurring depression, trauma, and anxiety frequently complicate treatment and increase relapse risk.
Classification
- Mild: Early harmful pattern with lower symptom burden.
- Moderate: Clear role dysfunction and persistent use despite consequences.
- Severe: High dependence burden with recurrent withdrawal and major impairment.
- Drinking-pattern descriptors: Harmful drinking (ongoing harm), at-risk drinking (hazard-prone context), hazardous drinking (high-likelihood harm), and intoxication (acute psycho-behavioral impairment).
- Withdrawal time-course cues: Mild symptoms often begin 6-24 hours after last drink and usually improve within 1-2 days; moderate-to-severe symptoms may persist up to about 6 days. Hallucinations commonly emerge around 12-24 hours, seizures around 6-48 hours, and withdrawal delirium around 72-96 hours.
- Remission milestones: Early remission after at least 3 months and less than 12 months without full active criteria; sustained remission after at least 12 months.
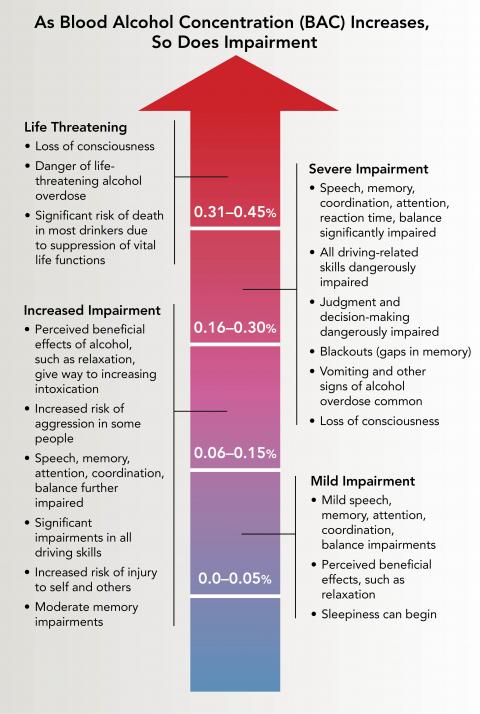 Illustration reference: OpenRN Nursing Mental Health and Community Concepts 2e Ch.14.2.
Illustration reference: OpenRN Nursing Mental Health and Community Concepts 2e Ch.14.2.
Nursing Assessment
NCLEX Focus
Track withdrawal trajectory over time; worsening autonomic signs and altered sensorium signal escalation risk.
- Assess pattern of use, last drink, prior detox history, and withdrawal complications.
- Obtain structured history domains: substance-use history, prior withdrawal treatment, prior treatment engagement, mental-health history, social history, and current medical symptoms.
- Assess for alcohol intoxication findings such as slurred speech, incoordination, unsteady gait, nystagmus, impaired attention/memory, and possible stupor/coma.
- Assess alcohol overdose red flags: inability to awaken, vomiting, seizures, slow or irregular breathing, slow heart rate, clammy skin, low temperature, and absent gag reflex.
- In suspected overdose, use high-risk breathing thresholds (fewer than 8 breaths/minute or pauses of 10 seconds or longer) as immediate escalation cues.
- Assess for co-ingestion of opioids, benzodiazepines, or other sedatives because combined CNS depression increases lethality and may change treatment priorities.
- Use screening prompts such as the Single Alcohol Screening Question (SASQ): “How many times in the past year have you had 4 (women) or 5 (men) or more drinks in a day?”
- If SASQ response is 1 or more, complete expanded AUD assessment and notify the provider for diagnostic follow-up.
- Use evidence-based alcohol tools as indicated (for example APQ, AUDIT, AUDIT-C, LDQ, SADQ) and track withdrawal severity with CIWA-Ar.
- Use CAGE as a rapid adjunct when indicated (Cut down, Annoyed, Guilty, Eye-opener); two or more “yes” answers warrant expanded diagnostic follow-up.
- Use CIWA-Ar as a symptom-triggered assessment tool; core domains include nausea/vomiting, tremor, sweats, anxiety/agitation, sensory disturbance, headache, and orientation.
- In protocol-based settings, recognize that CIWA-Ar scores below 10 often indicate no immediate medication requirement, with ongoing reassessment per agency policy.
- Assess vital signs, tremor, diaphoresis, agitation, orientation, and hallucination risk.
- Assess nutrition status and deficiency risk (especially thiamine depletion).
- Assess fall risk, seizure risk, aspiration risk, and suicidality.
- In adolescents, assess binge-drinking harms directly (school failure, legal/safety events, unprotected sex, violence exposure, and suicidal risk).
- In hospitalized settings, maintain high suspicion for underreported use and screen for withdrawal signs even when admission reason is nonpsychiatric.
- In perioperative or medical-surgical admissions, suspect withdrawal when abstinence reaches about 2 to 4 days and the patient develops tremor, anxiety, tachycardia, low-grade fever, or marked hypertension.
- Apply developmental-context assessment: adolescent risk behavior pattern, pregnancy risk counseling needs, and older-adult medication interaction risk.
Nursing Interventions
- Implement CIWA-Ar protocol and provide symptom-triggered medication administration.
- Maintain seizure precautions, close observation, and frequent reassessment intervals.
- Integrate fall-prevention controls (for example bed alarms and supervised mobility) when withdrawal confusion or agitation increases injury risk.
- Escalate rapidly for suspected withdrawal delirium (fluctuating cognition, severe agitation, fever, marked tachycardia/hypertension, or drenching sweats) due to high cardiopulmonary and fluid-electrolyte complication risk.
- Treat severe alcohol withdrawal as a medical emergency requiring high-acuity monitoring because mortality risk rises with hyperthermia, aspiration, cardiovascular instability, and major fluid-electrolyte derangements.
- Prioritize severe autonomic instability (especially marked hypertension) and notify the provider promptly while CIWA-Ar-guided withdrawal treatment is initiated.
- Treat suspected alcohol overdose as an emergency: activate EMS/911 and do not leave an unconscious person alone.
- Protect airway to reduce aspiration risk; keep the client partially upright or side-lying if vomiting risk is present.
- Recognize that BAC can continue to rise after drinking stops, so observation and serial reassessment are required even when the client appears to be “sleeping it off.”
- Support hydration, electrolyte correction, and nutritional replacement per orders.
- For moderate to severe intoxication, anticipate glucose/electrolyte monitoring, IV dextrose for hypoglycemia, thiamine replacement, and ICU escalation when airway or vital-sign instability is present.
- Avoid relying on activated charcoal or gastric lavage for isolated alcohol intoxication because rapid ethanol absorption limits benefit.
- Provide brief motivational counseling and referral planning for continuing care.
- Perform routine alcohol-use questioning for all clients, including pregnant clients, and use nonjudgmental discussion of perceived benefits/harms to start behavior-change counseling.
- Engage family/support systems when clinically appropriate.
- Offer mutual-aid linkage options (for example AA for clients and Al-Anon/Alateen for family members) to strengthen long-term recovery support.
- Reinforce that early screening and treatment of AUD improves outcomes for both the client and affected family members.
- Provide family-centered counseling that adolescent binge drinking can disrupt neurodevelopment and increase risks for injury, alcohol poisoning, and later substance-misuse progression.
- Counsel that no amount of alcohol is considered safe during pregnancy and link to prenatal-risk prevention support when relevant.
Alcohol Withdrawal Emergency
Untreated withdrawal may progress to seizures and delirium tremens; escalate care immediately for severe autonomic instability or fluctuating cognition.
Pharmacology
FDA-approved medications for AUD treatment include naltrexone, acamprosate, and disulfiram. Withdrawal treatment uses benzodiazepines (for example diazepam, lorazepam, or chlordiazepoxide) as first-line therapy to prevent seizures and delirium-tremens, with anticonvulsants in selected cases.
For disulfiram initiation, clients generally need to be abstinent from alcohol for at least about 12 hours before the first dose. Because disulfiram reactions can persist after discontinuation, alcohol should still be avoided for up to about 2 weeks after the last dose.
Disulfiram reactions can be triggered by unexpected ethanol sources (for example some liquid products or fermented drinks such as kombucha). Key interaction checks include metronidazole, isoniazid, phenytoin, and warfarin pathways.
Lorazepam is commonly used in CIWA-Ar symptom-triggered withdrawal protocols; chlordiazepoxide may still be used in selected settings but its long half-life can increase accumulation and oversedation risk, especially if relapse or concurrent CNS depressants occur.
Haloperidol may be used only as an adjunct in selected severe-agitation contexts because it does not treat the core withdrawal mechanism and can lower seizure threshold.
In ICU-level withdrawal care, dexmedetomidine may be used as an adjunct for sympathetic overactivity but does not prevent withdrawal seizures and requires close monitoring.
Nurses commonly administer thiamine and monitor electrolytes to reduce neurologic complications, including wernickes-encephalopathy progression risk. Ongoing medication adherence and relapse-prevention teaching remain central after stabilization.
In severe intoxication, treatment commonly includes BAC and co-ingestion evaluation, IV dextrose for hypoglycemia, and IV thiamine with dextrose for coma. If chemical sedation is required for severe agitation, benzodiazepines are used cautiously because alcohol-related respiratory depression can worsen.
Clinical Judgment Application
Clinical Scenario
A hospitalized client with escalating wine intake develops anxiety, tremor, sweating, headache, and increasing CIWA-Ar score.
- Recognize Cues: Rising autonomic signs, visible tremor, and worsening anxiety.
- Analyze Cues: Findings are consistent with active alcohol withdrawal.
- Prioritize Hypotheses: Prevent seizure, delirium, and cardiopulmonary deterioration.
- Generate Solutions: Continue symptom-triggered protocol, safety precautions, and hydration support.
- Take Action: Administer prescribed withdrawal medication and re-evaluate CIWA-Ar response.
- Evaluate Outcomes: Confirm symptom reduction, stable vitals, and readiness for step-down treatment.
Related Concepts
- substance-use-disorders - Broad framework for diagnosis, dependence, and relapse risk.
- dealing-with-addiction - Details continuum care and overdose/withdrawal management.
- stimulant-use-disorders - Contrasts withdrawal patterns and overdose response.
- opioid-use-disorder - Shares detox and long-term recovery planning challenges.
- therapeutic-communication-and-relationships - Supports engagement in behavior change.