Burn Injury Assessment Resuscitation and Complications
Key Points
- Burn severity is driven by depth, etiology, and total body surface area (TBSA).
- Early priorities include hazard removal/decontamination, airway protection, and fluid resuscitation.
- Global and U.S. burn burden remains high (about 180,000 annual deaths worldwide and about 486,000 injuries yearly in the United States in recent estimates).
- The Rule of Nines and palmar method support rapid TBSA estimation and triage.
- Larger TBSA burden (for example >30% in many adult contexts) sharply increases burn-shock and organ-failure risk.
- Even lower TBSA burdens can destabilize volume status; hypovolemic shock risk rises with clinically significant burn size and capillary leak.
- Major respiratory risk includes inhalation injury from heat, smoke particulates, and toxic gases (for example carbon monoxide/cyanide exposure).
- Depth classes differ by pain, blanching, tissue appearance, and expected healing duration.
- High-risk complications include inhalation injury, hypovolemic shock, infection/sepsis, thermoregulation failure, contractures, and psychological trauma.
- Topical anti-infective burn therapy commonly uses silver sulfadiazine or mafenide acetate with strict aseptic application and systemic-absorption surveillance.
Pathophysiology
Burn injury disrupts skin barrier, microvascular integrity, and systemic inflammatory balance. With larger burns, capillary leak and fluid shifts reduce effective intravascular volume and can rapidly cause tissue hypoperfusion.
Early tissue response is often described in concentric injury zones: central coagulation (irreversible necrosis), surrounding stasis (salvageable but hypoperfused tissue), and outer hyperemia (reversible perfusion change).
Depth and etiology alter local tissue destruction and downstream complications. Thermal, chemical, electrical, and radiation injuries require distinct safety and treatment considerations.
Severe burns can produce long-duration morbidity beyond initial closure, including functional, psychosocial, and chronic health impacts. Recovery burden is often amplified in populations with limited prevention resources or reduced access to specialty burn care.
Classification
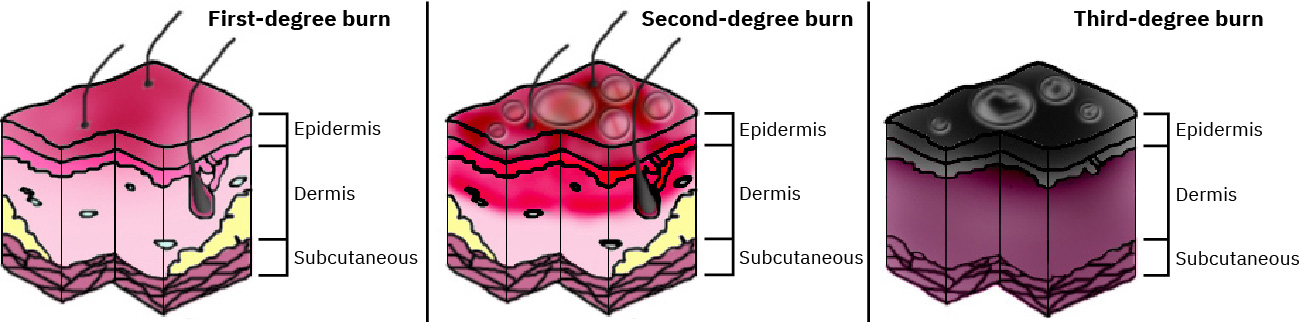 Illustration reference: OpenStax Clinical Nursing Skills Ch.8.
Illustration reference: OpenStax Clinical Nursing Skills Ch.8.
- Depth class:
- superficial (first-degree): epidermis only; erythematous pink-red dry skin without blisters, mild-to-moderate pain, and expected healing without scarring
- partial-thickness (second-degree): epidermis + dermis involvement with moist blistered blanchable erythema, moderate-to-severe pain, and healing over weeks depending on depth
- full-thickness (third-degree): epidermis and dermis fully destroyed into subcutaneous tissue; white/black/brown dry leathery nonblanchable tissue with possible eschar and minimal pain due to nerve destruction
- fourth-degree (described in some systems): extends into muscle/bone; life-threatening with high amputation risk
- Cause class:
- thermal: scald, dry-heat/flame/radiant, contact, and extreme-cold tissue-freeze injuries
- chemical:
- acids: often localized coagulation-type injury
- alkalis: deeper progressive liquefaction necrosis with prolonged tissue damage risk
- oxidizers/miscellaneous agents: mixed skin and systemic toxicity patterns
- electrical: entry/exit injury pattern with deeper internal tissue-path damage possible
- radiation: alpha/beta/gamma exposure with depth and systemic impact differences
- Burden class: TBSA involvement using Rule of Nines or palmar estimate.
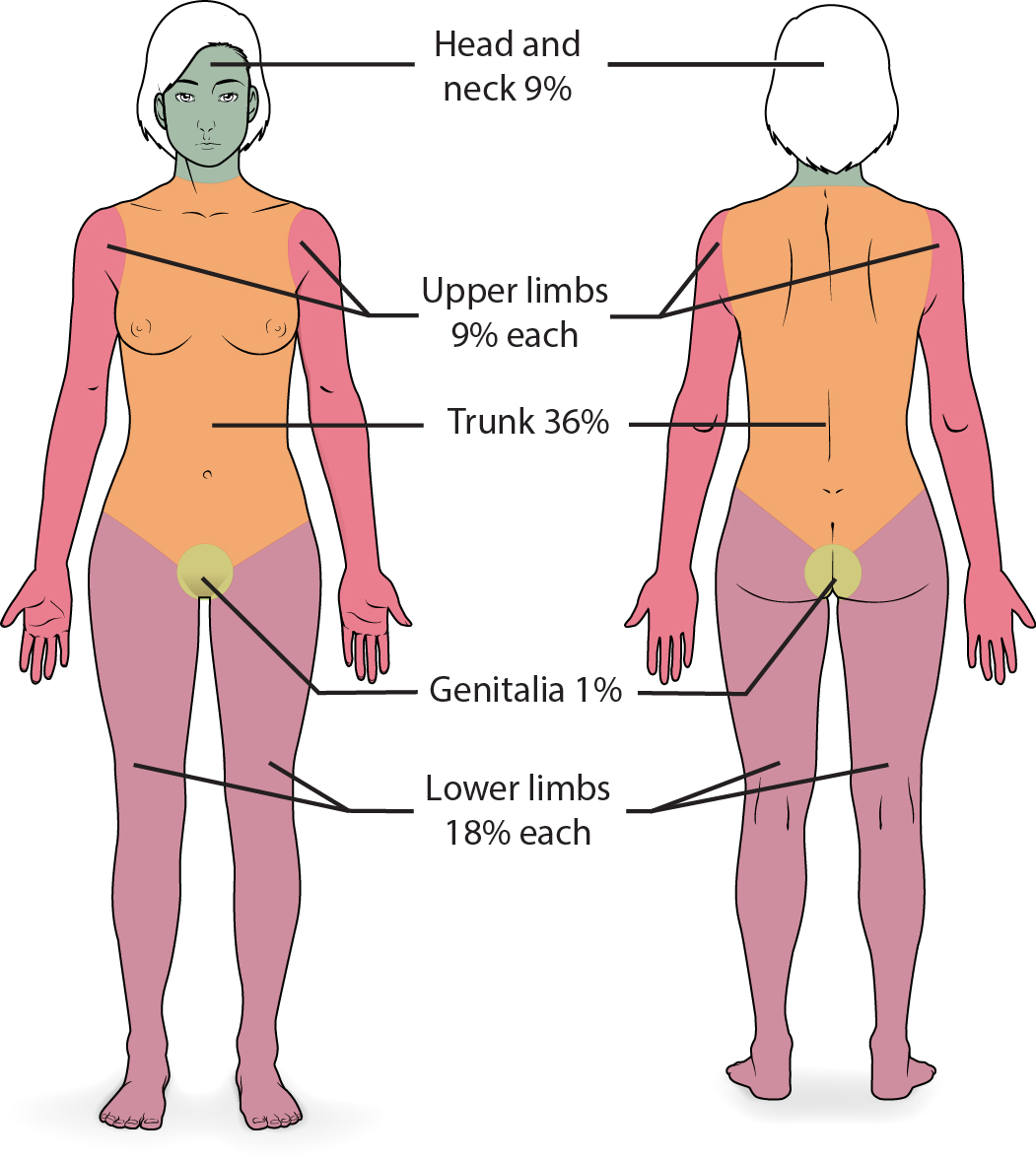 Illustration reference: OpenStax Clinical Nursing Skills Ch.8.
Illustration reference: OpenStax Clinical Nursing Skills Ch.8.
- Rule of Nines quick-map (adult): head 9%, each arm 9%, anterior trunk 18%, posterior trunk 18%, each leg 18%, perineum 1%
- Palmar estimate: palm without fingers is about 0.5% TBSA; palm with fingers is about 1% TBSA
- Treatment TBSA calculation usually counts only partial- and full-thickness burned areas.
- Severe-burn threshold often starts around >20% TBSA in adults and >10% TBSA in children.
- Physiologic risk class: Airway/inhalation risk, shock risk, infection risk, and functional recovery risk.
- Transfer-acuity class: Consider burn-center transfer for larger TBSA burden (often >10%), full-thickness injury, burns involving face/hands/feet/genitalia/major joints, chemical or electrical etiology, or associated trauma.
Nursing Assessment
NCLEX Focus
Prioritize ABCs, exposure context, and early hemodynamic compromise signs before detailed local care.
- Assess burn depth and pattern, including entry/exit evidence in suspected electrical injury.
- In superficial burns, assess skin-tone-specific color changes (for example pink-red in lighter skin and reddish-brown change in darker skin).
- Identify etiology explicitly because management differs by mechanism (for example chemical decontamination priorities versus thermal injury support).
- In thermal injuries, assess exposure type and duration (for example scald versus dry heat/flame) because mechanism commonly predicts depth and surgery risk.
- Estimate TBSA promptly and repeat as edema and demarcation evolve.
- Use an ABCDE emergency sequence in initial triage, with airway and breathing stabilization completed before detailed local wound work.
- Treat high TBSA burden as a shock-risk trigger and escalate hemodynamic surveillance early.
- Use patient-appropriate pain tools during triage and reassessment (numeric scale when possible; observational scales such as FACES or PAINAD when communication is limited).
- Monitor for burn-related hypovolemic shock when TBSA burden is clinically significant (commonly >10% risk context in many adult pathways).
- Screen for inhalation injury (head/neck/chest burns, smoke exposure, airway irritation signs).
- In full-thickness injury, continue pain assessment because mixed-depth patterns (coexisting partial-thickness zones) can still produce substantial pain.
- Differentiate inhalation-injury patterns when suspected:
- systemic toxic exposure (for example carbon monoxide/cyanide)
- thermal upper-airway injury
- chemical injury involving upper and lower airways
- Monitor perfusion and volume status: urine output, vital trends, mentation, and shock indicators.
- Diagnose most first-degree burns clinically; additional laboratory testing is often unnecessary unless other instability features are present.
- For deeper or extensive partial-thickness injury, anticipate broader diagnostics (for example CBC, CMP, ABG, and smoke-inhalation-directed chest imaging/cardiac testing as ordered).
- For chemical burns, identify specific agent and concentration and verify whether injury can progress after apparent surface decontamination.
- For electrical burns, assess entry/exit sites and evaluate internal-injury risk between those points (arrhythmia, muscle injury, renal complications, trauma from falls).
- For radiation exposure patterns, assess for systemic toxicity signs and acute radiation syndrome risk when exposure burden is high.
- Assess social-risk context (for example housing instability, poverty, language/access barriers) that may affect prevention, follow-up, and long-term recovery.
- Assess long-term psychological burden (depression, anxiety, trauma symptoms, quality-of-life decline), even when cutaneous healing appears complete.
Nursing Interventions
- Remove exposure source and complete decontamination first for chemical/radiation cases.
- Use immediate copious irrigation for most external chemical exposures while confirming agent-specific exceptions per toxicology/provider guidance.
- Complete required decontamination before interfacility transfer when contamination is ongoing risk.
- Protect airway early when inhalation injury is suspected; anticipate rapid deterioration.
- Begin fluid resuscitation per protocol and titrate to urine output and perfusion goals.
- After airway and breathing stabilization, prioritize IV access and early volume support because burn-related fluid losses can rapidly destabilize perfusion.
- In larger burns (commonly >=20% TBSA), initiate formal burn-resuscitation protocol early, often using Parkland-based planning with urine output endpoint commonly >0.5 mL/kg/hr.
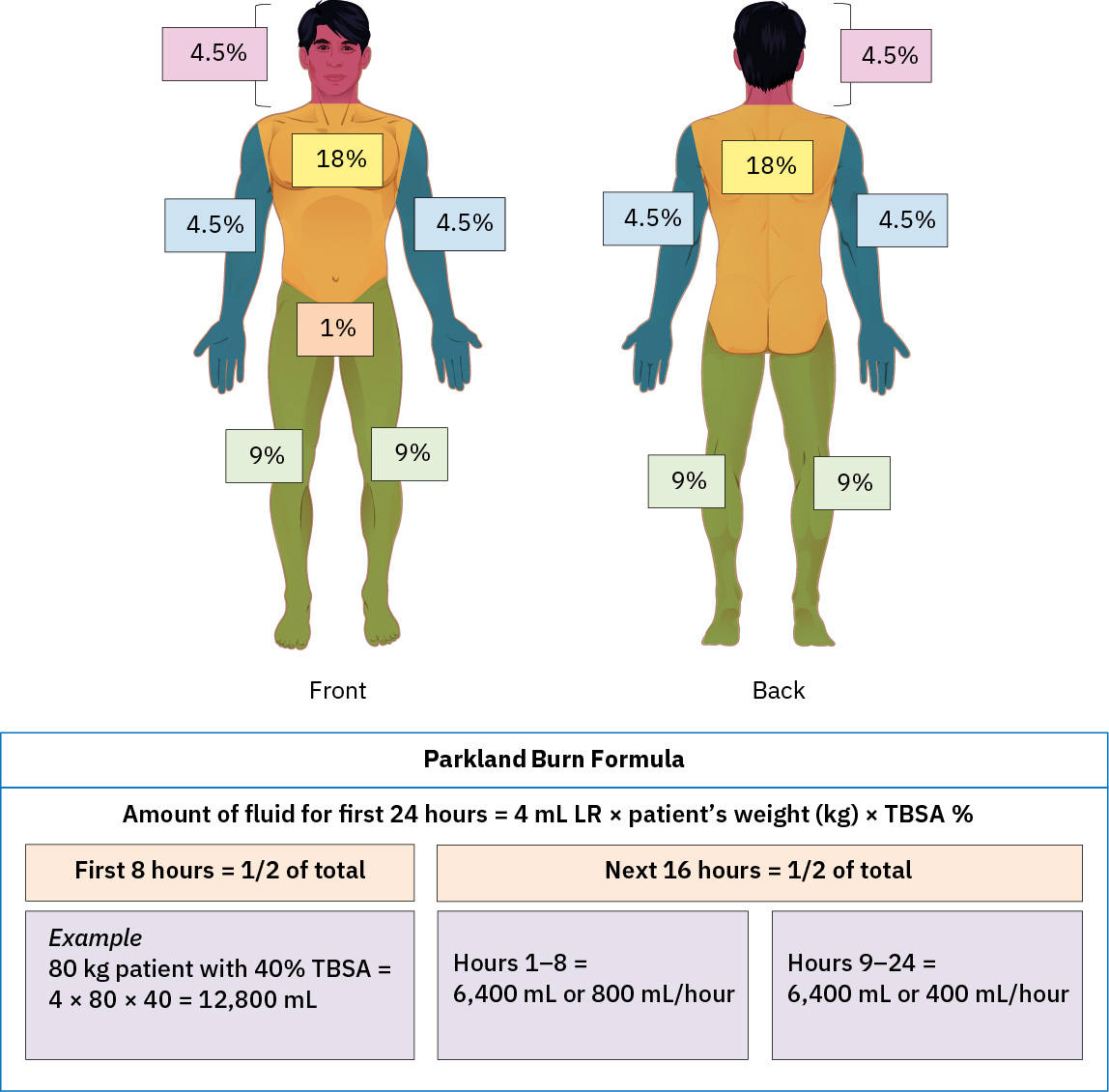 Illustration reference: OpenStax Clinical Nursing Skills Ch.8.
Illustration reference: OpenStax Clinical Nursing Skills Ch.8. - Recognize that larger partial-thickness burden (for example >20% TBSA) can trigger systemic inflammatory response with hypovolemic or septic-shock progression risk.
- Remove clothing and jewelry near burn zones early to reduce constriction and retained heat burden.
- For partial-thickness wound care, combine cooling/cleansing with nonadherent dressings and ordered topical agents (for example silver sulfadiazine or mupirocin).
- For localized second- and third-degree burns, apply ordered topical anti-infectives (for example silver sulfadiazine or mafenide acetate) with gloves and aseptic technique.
- Maintain full cream coverage of treated burn surfaces per order to reduce bacterial colonization risk.
- Avoid occlusive dressings over topical burn anti-infectives unless specifically ordered because occlusion increases systemic absorption risk.
- Monitor for hypersensitivity and systemic-absorption effects during therapy, including renal trend monitoring (for example creatinine) when body-surface exposure is substantial.
- Avoid applying silver sulfadiazine near mucosal or ocular areas when possible and use extra caution on large body-surface areas.
- Verify contraindication risk before silver sulfadiazine: sulfa allergy, near-term pregnancy status, and premature/newborn age under 2 months.
- Premedicate for painful wound care when ordered (commonly around 30 minutes before dressing changes) and reassess pain before/during/after procedures.
- For electrical injuries, include early ECG/cardiac rhythm surveillance and monitor for rhabdomyolysis-associated renal injury.
- Coordinate multidisciplinary burn care, including surgery, respiratory support, wound/pain management, rehabilitation, nutrition, psychosocial care, and discharge reintegration planning.
- For scar/contracture prevention, coordinate early physical/occupational therapy, splinting, and reconstructive pathways (for example skin graft planning) when indicated.
- In extensive burns (for example >40% TBSA), monitor closely for thermoregulation failure and hypothermia risk.
- Intensify infection-prevention bundle: strict hand hygiene/PPE discipline, protective isolation considerations, topical antimicrobial strategies, and culture-based escalation when concerns arise.
- Escalate suspected wound infection promptly when fever, progressive erythema, or yellow foul-smelling drainage appears.
- In circumferential or deep burns, monitor for evolving compartment syndrome (for example severe pain, swelling, paresthesia, pulse changes, pallor) and escalate urgently.
- Reinforce burn-prevention teaching for high-risk settings (for example home heat sources, occupational chemical exposure, farm fertilizer handling).
- Integrate early and recurring mental-health support because postburn depression, anxiety, and PTSD can persist and delay functional reintegration.
- For minor burns, apply a structured local-care sequence:
- cool (tap water or saline)
- clean (mild soap/water)
- cover (topical antimicrobial and dressing strategy per order/policy)
- comfort (analgesia and positioning/splint support as indicated)
- blister strategy: large blisters are commonly debrided per order/policy, while selected small or function-critical blisters may be left intact
- Manage uncomplicated first-degree burns in outpatient settings when no airway, perfusion, or high-risk exposure concerns are present.
- Expect uncomplicated first-degree burns to re-epithelialize in roughly 5-10 days with minimal long-term sequelae.
- Expect many uncomplicated second-degree burns to heal in about 3 weeks, with scarring risk increasing as dermal depth increases.
- Treat all third-degree burns as high acuity regardless of size and coordinate urgent burn-center level care and graft-planning pathways.
- Plan for prolonged third-degree recovery: healing often requires at least 8 weeks and can extend to months or years with permanent scar burden.
Burn Shock Window
Delayed recognition of fluid shift and airway compromise can cause rapid multisystem decline.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| intravenous-fluid-categories-tonicity-and-infusion-regulation (iv-fluids) | Lactated Ringer’s | Use burn-resuscitation protocols and monitor urine output/perfusion endpoints. |
| topical-antibiotic-therapy | Silver sulfadiazine, mafenide, mupirocin | Apply with aseptic technique and nonocclusive dressing strategy; monitor hypersensitivity and systemic-absorption effects. |
| analgesics | Opioid and nonopioid regimens | Titrate to severe procedural/background pain while monitoring respiratory risk. |
Clinical Judgment Application
Clinical Scenario
A patient presents after a house fire with partial- and full-thickness burns over the torso and upper extremity, hoarse voice, and progressive tachycardia.
- Recognize Cues: High TBSA burden plus airway and perfusion warning signs.
- Analyze Cues: Combined inhalation risk and capillary-leak fluid loss increase decompensation risk.
- Prioritize Hypotheses: Airway compromise and evolving burn shock are immediate threats.
- Generate Solutions: Activate burn pathway, secure airway strategy, initiate resuscitation, and transfer coordination.
- Take Action: Implement protocolized monitoring and interdisciplinary escalation.
- Evaluate Outcomes: Urine output and perfusion stabilize, and respiratory status remains controlled.
Related Concepts
- wound-classification-framework - Burn injury is a wound mechanism with distinct severity implications.
- wound-healing-phases-and-closure-intentions - Burn depth affects healing trajectory and closure planning.
- delayed-wound-healing-factors-and-complications - Large burns have elevated infection and delayed-healing risks.
- fluid-volume-deficit-hypovolemia-and-dehydration - Burn-related capillary leak can produce severe hypovolemia.
- acute-vs-chronic-pain-and-observable-cues - Burn recovery often requires layered pain management strategies.
- stevens-johnson-syndrome-and-toxic-epidermal-necrolysis - Severe epidermal-loss syndrome that can mimic partial-thickness burn patterns.
Self-Check
- How do depth and TBSA jointly determine burn acuity?
- Which cues should trigger aggressive airway planning in burn patients?
- Why is urine output a key early endpoint during burn resuscitation?