Wound Healing Phases and Closure Intentions
Key Points
- Wound healing follows hemostasis, inflammatory, proliferative, and maturation phases.
- Primary intention heals fastest with approximated edges and less scarring.
- Secondary intention requires granulation-based fill-in and has longer healing time.
- Tertiary intention is delayed closure after edema or infection burden is controlled, commonly after about 3-5 days of monitored open management.
Pathophysiology
After tissue injury, healing begins immediately with hemostasis and progresses through inflammation, proliferation, and maturation. Hemostasis includes early vasoconstriction, clotting-factor activation, and platelet growth-factor signaling, and commonly lasts up to about 60 minutes depending on injury severity. Keratinocytes, fibroblasts, vascular endothelial cells, and immune cells jointly support inflammatory control, cell migration, and angiogenesis across the healing cascade.
Some clinical frameworks describe three phases by treating hemostasis as an early component of the inflammatory phase. In bedside documentation, both three-phase and four-phase language may appear; phase interpretation should stay consistent within the care team.
Inflammatory-phase findings are typically edema, erythema, and exudate as leukocytes enter the wound bed for cleanup and bioburden control. Exudate refers to wound fluid drainage (for example serous or purulent output). This phase usually continues for about 3-7 days, with neutrophils, macrophages, lymphocytes, and mast cells coordinating early wound-bed cleanup.
The proliferative phase commonly begins around day 3 or 4 and may continue for weeks. Collagen production typically peaks around days 5-7, capillary growth forms fragile granulation tissue, and epithelial migration advances wound closure. By about the end of week 2, inflammatory-cell burden usually declines and generalized inflammatory symptoms should lessen if healing is progressing normally. In primary-intention closure, epithelial sealing can occur within about 24-48 hours, so visible granulation tissue may be minimal or not evident.
The maturation phase often starts around day 21 and may continue for months to years. Scar tissue strengthens through collagen remodeling but does not fully regain original tissue properties.
Closure method changes expected timeline and scar burden. Primary-intention wounds are closed with sutures, staples, adhesive, or other approximation methods so healing proceeds beneath closed edges. Wounds with tissue loss or nonapproximated edges rely on prolonged granulation and remodeling.
Classification
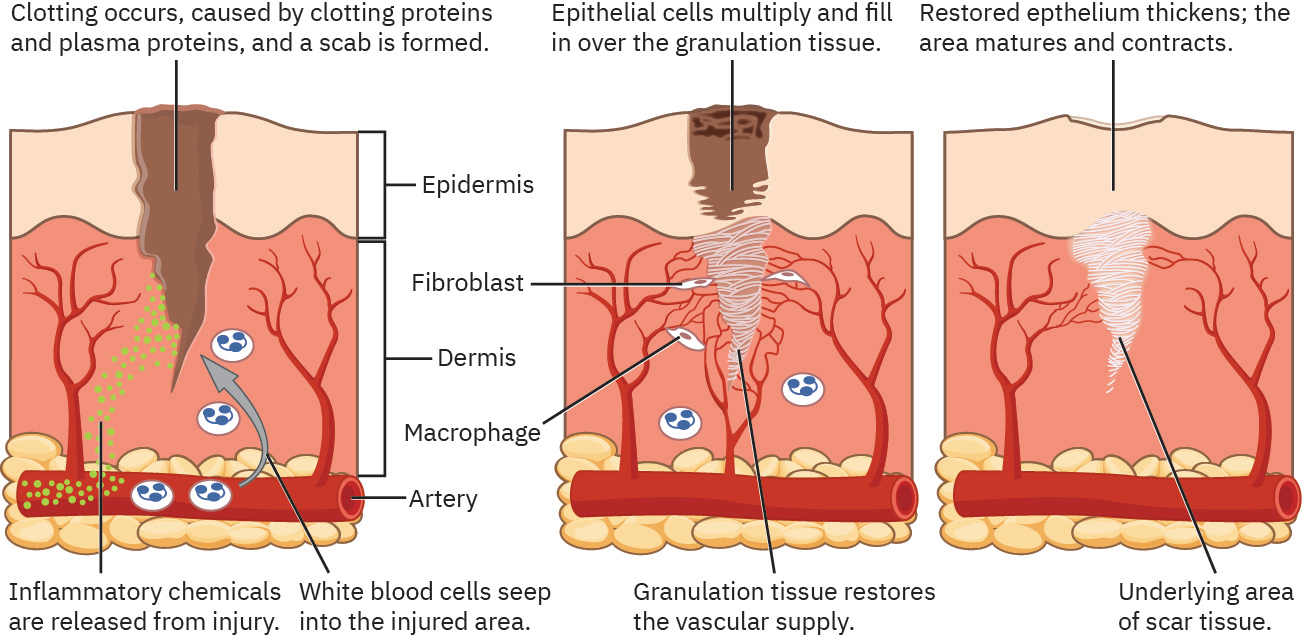 Illustration reference: OpenStax Clinical Nursing Skills Ch.8.
Illustration reference: OpenStax Clinical Nursing Skills Ch.8.
- Hemostasis: Vasoconstriction, fibrin clot formation, and early protective matrix.
- Inflammatory phase (about days 0-7): Phagocytosis, leukocyte activity, and local inflammatory signs.
- Proliferative phase (about day 3/4 through weeks): Collagen synthesis, angiogenesis, granulation tissue, and epithelialization.
- Maturation phase (from about day 21 to months/years): Collagen reorganization with scar strengthening; tissue remains less elastic and not as strong as preinjury skin.
- Maturation sequelae: Scar tissue may not sweat, tan, or regrow hair normally; scars crossing joints can contribute to arthrofibrosis and mobility loss.
- Primary intention: Clean-edged wound with approximated closure.
- Secondary intention: Nonapproximated wound that fills from the bottom up with granulation tissue.
- Tertiary intention: Delayed closure after an open period (commonly about 3-5 days) due to swelling, infection concern, or need for drainage before closure.
Nursing Assessment
NCLEX Focus
Questions commonly test whether observed findings match expected phase timing and whether closure method predicts slower progression.
- Match wound appearance with expected phase and timing trends.
- Assess wound-edge approximation, tissue loss extent, and granulation quality.
- Identify wound-healing intent and expected risk pattern:
- primary intention: lower contamination risk when closure remains intact
- secondary intention: higher contamination/infection risk; needs strong protection
- tertiary intention: delayed closure context with prolonged healing and scar risk
- Differentiate healthy versus unhealthy granulation tissue:
- healthy: pink, moist, fragile, and usually not painful
- unhealthy: dark red, painful, easily bleeding, or covered by white/yellow biofilm-like tissue
- Identify suspicious biofilm or unhealthy granulation and escalate for trained-provider debridement/culture decisions.
- Monitor for stalled progression, recurrent inflammation, or delayed epithelialization.
- Escalate if expected timeline is absent (for example persistent inflammatory dominance past early phase or lack of progressive epithelialization by week 2 trend checks).
- Evaluate strain risk on closure lines from coughing, lifting, or poor movement support.
- Assess scar-related mobility restriction risk near joints because dense remodeling can limit range of motion.
Nursing Interventions
- Protect fresh closures from mechanical strain during early healing.
- Maintain moist, clean wound environment that supports epithelial migration.
- Protect secondary-intention wounds from contamination and trauma while granulation fills the wound bed.
- For tertiary-intention trajectories, reassess readiness for delayed closure as swelling or infection resolves.
- Coordinate nutrition and oxygenation support to optimize proliferation and remodeling.
- Escalate wounds that fail expected progression or show persistent inflammatory dominance.
- For wounds across high-motion joints, plan early mobility-preserving strategies to reduce scar contracture-related stiffness.
False-Progress Assumption
Reduced surface redness alone does not confirm adequate deep healing; continue phase-based reassessment.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| analgesics | Acetaminophen, ibuprofen | Improve tolerance for wound care and mobility while monitoring adverse effects. |
| corticosteroids (steroids) | Prednisone-class agents | Can blunt inflammatory response and contribute to delayed healing risk. |
Clinical Judgment Application
Clinical Scenario
A postoperative patient has a sutured abdominal incision with increasing strain from repeated coughing episodes.
- Recognize Cues: Early closure under frequent mechanical stress.
- Analyze Cues: Primary intention healing may be compromised by tension on unhealed tissue.
- Prioritize Hypotheses: Highest risk is disruption of closure and delayed healing trajectory.
- Generate Solutions: Support splinting, optimize pain control, reduce strain during movement, and reassess wound integrity.
- Take Action: Implement protective strategies and monitor for signs of closure compromise.
- Evaluate Outcomes: Incision remains approximated and advances through expected healing phases.
Related Concepts
- wound-classification-framework - Classification predicts expected healing pathway.
- delayed-wound-healing-factors-and-complications - Local and systemic barriers can stall phase progression.
- wound-management-interventions-and-adjunctive-therapies - Intervention selection influences whether phase progression is restored.
- pressure-injury-staging-and-risk-assessment - Pressure injury healing often follows prolonged secondary intention.
- nutrition-related-laboratory-and-diagnostic-tests - Protein and metabolic status influence tissue repair capacity.
- documenting-and-reporting-data - Phase-consistent documentation improves trend detection.
Self-Check
- Which phase findings indicate progression from inflammation to proliferation?
- Why does secondary intention generally require longer healing than primary intention?
- When is tertiary intention selected instead of immediate closure?