Assisting With Sensory Deficits
Key Points
- Sensory deficits increase fall risk and communication barriers across care settings.
- Safety improves when environment is consistent, clutter-free, and adapted to the resident’s deficit pattern.
- Hearing and speech support require slower pacing, visual cues, and individualized communication tools.
Pathophysiology
Sensory deficits reduce environmental input needed for balance, hazard recognition, and social interaction. Age-related changes and neurologic disease can impair vision, hearing, and speech processing simultaneously.
Visual deficits (for example cataracts, glaucoma, macular degeneration) affect acuity, peripheral vision, or central-field detail, changing navigation safety. Hearing loss reduces speech discrimination and emergency-signal awareness.
Speech impairment and aphasia after brain injury can increase frustration, isolation, and behavioral escalation when communication demands exceed processing capacity.
Classification
- Visual impairment: Depth-perception problems, cataracts, glaucoma, or macular degeneration that alter navigation safety.
- Hearing impairment: Age-related presbycusis and hearing-aid dependent communication needs.
- Kinesthetic impairment: Reduced touch/pressure/vibration/position sense (for example peripheral neuropathy) that impairs fine motor function and balance.
- Speech impairment: Expressive/receptive aphasia and slowed language processing.
- Communication supports: Whiteboards, communication books, gestures, touch cues, and environmental cueing.
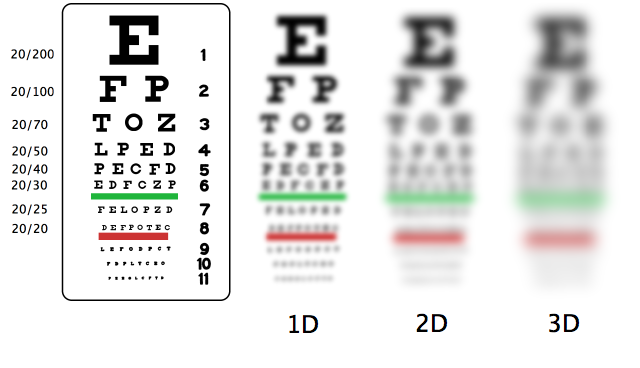 Illustration reference: OpenRN Nursing Assistant Ch.9.7.
Illustration reference: OpenRN Nursing Assistant Ch.9.7.
Nursing Assessment
NCLEX Focus
Priority questions focus on immediate environmental modifications and communication strategies that reduce injury risk.
- Assess ability to detect obstacles, read cues, and locate essential items safely.
- Evaluate hearing-aid function, battery status, fit, and cleaning needs.
- Confirm hearing-aid maintenance workflow (for example weekly battery change or nightly charging for rechargeable models) and safe storage to prevent loss.
- Verify hearing-aid handling safety habits: remove/turn off battery power when devices are not in use, avoid water exposure, and use dry-cloth cleaning methods.
- Observe communication effectiveness and frustration triggers during care.
- Assess for neuropathy-pattern symptoms (burning, tingling, numbness, reduced vibration/position sense) that increase gait instability and self-care difficulty.
- Monitor for isolation, agitation, or aggression that may reflect unmet communication needs in aphasia or hearing loss.
- Report sudden changes in sensory function, increased confusion, or new safety incidents.
Nursing Interventions
- Maintain consistent room layout with clear pathways and adequate lighting.
- In unfamiliar settings, provide explicit room-layout orientation with tactile boundary landmarks for low-vision residents who rely on touch-based navigation.
- Ensure prescribed eyeglasses/hearing aids are clean, fitted, and available.
- Reinforce use of low-vision aids (for example magnifiers, large-print materials, and adaptive technologies) to preserve functional independence.
- During bathing or water-exposure activities, remove hearing aids, store them in a labeled protective case, and restore them promptly afterward.
- Identify yourself when entering the space of a client with visual impairment and verbally orient to your role before care tasks.
- Keep call light and frequently used personal items in consistent, clearly described locations before leaving the room.
- During assisted ambulation, give advance verbal cues when approaching objects or environmental hazards.
- Avoid unnecessary room rearrangement and describe environmental layout changes before movement/activity.
- Use clock-face orientation for meal trays and high-contrast labeling for frequently used items when appropriate.
- Face resident directly when speaking; use simple phrasing, gestures, and gentle touch cues.
- Reduce background noise when possible and reinforce that hearing aids amplify sound but may not restore speech clarity in noisy spaces.
- Reinforce device-care basics: dry soft-cloth cleaning, no internal-canal probing with objects, and battery preservation when devices are off-body.
- Do not assume nodding or smiling indicates comprehension; verify understanding with brief teach-back or simple response checks.
- Provide extra processing time and avoid rushing responses in aphasia.
- Use communication boards/books for residents with speech-expression limits.
- Use whiteboards or other written supports when cognition permits and follow speech-therapy communication plans.
- For severe hearing impairment, document and communicate preferred method (for example verbal, written, lipreading, or ASL) in the care plan.
- In hospitalized older adults, prioritize access to usual glasses/hearing aids because missing sensory aids can worsen deprivation and delirium risk.
- Coordinate audiology, speech-language pathology, and interpreter pathways when communication barriers persist despite baseline accommodations.
- Teach patients and families about available hearing-support organizations or peer-support resources to strengthen long-term self-advocacy.
- Coordinate referral to vision-rehabilitation services for home safety modification and navigation training when persistent visual deficits affect ADLs.
- Include family/caregivers in visual-impairment teaching to align support with the patient’s goals and home routine.
Sensory-Barrier Injury Risk
Unaddressed sensory deficits can cause preventable falls, communication failure, and escalating distress behaviors.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| ototoxic-medications | Hearing-risk medication contexts | New hearing decline during treatment should be reported promptly. |
| sedatives | Anxiety/sleep management contexts | Sedation can worsen sensory-processing limits and increase fall risk. |
Clinical Judgment Application
Clinical Scenario
A resident with glaucoma and hearing loss starts bumping into furniture, misses call-light location, and becomes agitated during rushed care interactions.
- Recognize Cues: Combined sensory barriers, navigation difficulty, and communication frustration.
- Analyze Cues: Environmental setup and communication style are not matching resident needs.
- Prioritize Hypotheses: Immediate priority is fall-risk reduction and communication adaptation.
- Generate Solutions: Clear pathway, improve lighting, verify hearing aids, use front-facing communication and slower pacing.
- Take Action: Reorganize environment and implement cue-based interaction plan.
- Evaluate Outcomes: Resident navigates more safely and agitation decreases.
Related Concepts
- fall-prevention - Sensory adaptation is a core component of individualized fall-risk management.
- communication-process - Effective communication methods must match sensory and language limitations.
- caring-for-clients-with-dementia - Sensory deficits can amplify confusion and behavioral symptoms.
- promoting-independence-during-adls - Adaptive tools support safe participation despite deficits.
- documenting-and-reporting-data - Objective reporting of sensory changes guides plan updates.
Self-Check
- Which environmental changes are most important for severe visual impairment?
- How should communication be modified for residents with aphasia?
- Why must hearing-aid maintenance be part of daily safety support?