Gastroesophageal Reflux Disease GERD
Mahahalagang Punto
- Ang GERD ay talamak na backflow ng laman ng tiyan papunta sa esophagus.
- Karaniwan ang disease burden sa adults at maaaring umusad mula symptom-only reflux tungo sa mucosal injury.
- Kabilang sa core risk factors ang lower-esophageal-sphincter dysfunction, hiatal hernia, delayed gastric emptying, obesity, tobacco/alcohol use, pagbubuntis, at piling medications.
- Prayoridad sa nursing ang symptom control, risk-factor modification, at pag-iwas sa erosive o premalignant esophageal complications.
Pathophysiology
Nagkakaroon ng GERD kapag paulit-ulit na nadidikit ang refluxed gastric contents sa esophageal mucosa dahil humihina ang normal antireflux barriers. Ang lower-esophageal-sphincter tone abnormalities, pressure-related anatomy changes (halimbawa hiatal hernia), delayed gastric emptying, at impaired esophageal clearance mechanisms ay nagpapataas ng reflux exposure.
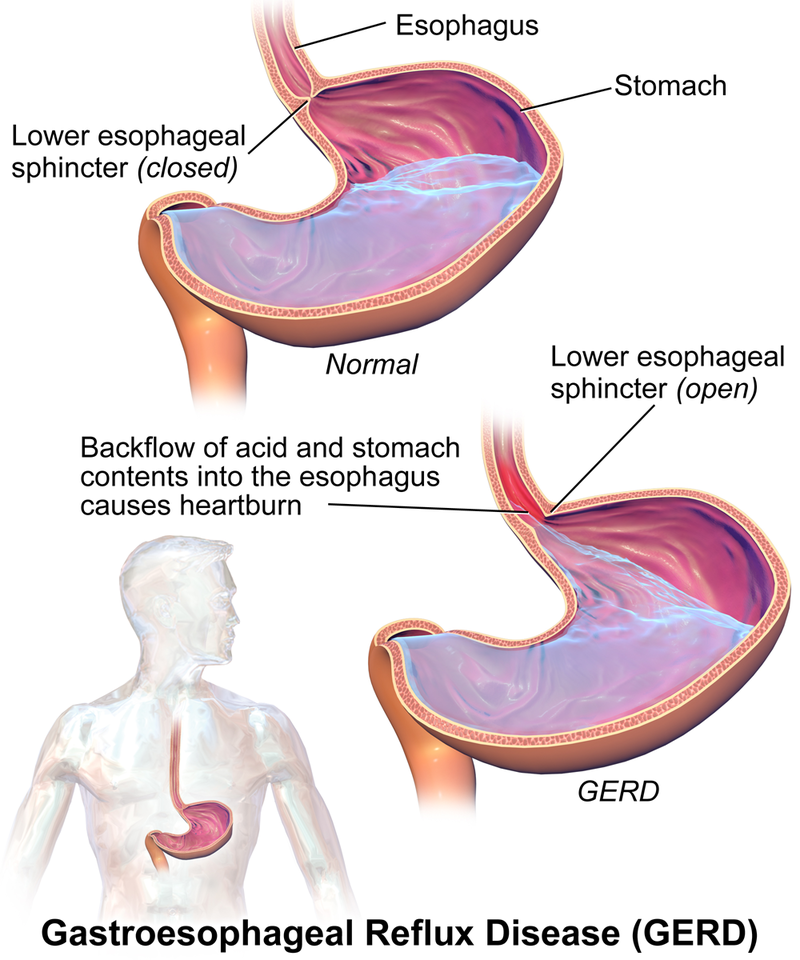 Illustration reference: OpenRN Nursing Pharmacology 2e Ch.7.3.
Illustration reference: OpenRN Nursing Pharmacology 2e Ch.7.3.
Karaniwang nalilinis ang refluxed acid sa pamamagitan ng esophageal peristalsis at bahagyang nababuffer ng salivary bicarbonate. Kapag humina ang depensang ito, naiipon ang mucosal injury. Ang patuloy na reflux ay maaaring umusad mula nonerosive symptoms tungo sa nakikitang esophageal injury at, sa ilang kliyente, metaplastic change risk.
Ang talamak na reflux injury ay maaaring magdulot ng pagpapalit ng normal squamous epithelium ng intestinal-type cells (Barrett pattern), na nagpapataas ng panganib ng esophageal adenocarcinoma sa paglipas ng panahon.
Classification
- Nonerosive reflux disease: Reflux symptoms na walang nakikitang esophageal erosion.
- Erosive esophagitis: Reflux na may erosions o ulceration ng esophageal mucosa.
- Barrett esophagus spectrum: Intestinal metaplasia risk state na kaugnay ng chronic reflux exposure.
Nursing Assessment
NCLEX Focus
Ihiwalay ang uncomplicated reflux symptoms sa mga cue ng progressive mucosal injury.
- Suriin ang tipikal na symptom pattern, kabilang ang postprandial o recumbent retrosternal burning (heartburn) at acid regurgitation.
- I-screen ang kaugnay na sintomas gaya ng dysphagia/odynophagia, nausea, epigastric pain, at frequent belching.
- Kilalanin ang atypical presentations, kabilang ang chronic cough, hoarseness/laryngitis, chest pain, bagong asthma pattern, at dental erosion concerns.
- I-screen ang risk factors kabilang ang central obesity, smoking, family history ng Barrett/esophageal cancer patterns, pagbubuntis, tobacco/alcohol use, age, socioeconomic constraints, at medication contributors.
- I-track ang functional impact at tugon sa lifestyle o medication measures sa paglipas ng panahon.
- Ihiwalay ang reflux chest pain mula sa posibleng cardiac ischemia presentations at mag-escalate ng cardiac-rule-out workflows kapag indicated.
- Suriin ang nutrition status at i-monitor ang aspiration-related cues (wheezing, chronic cough, hoarseness) at anemia risk kapag pinaghihinalaan ang erosive disease.
- Kilalanin na maaaring asymptomatic ang Barrett change at matukoy lamang sa endoscopy na ini-order para sa chronic reflux symptoms.
Diagnostics
- Clinical diagnosis/PPI trial: Maraming kliyente ang nade-diagnose batay sa history o sa symptom response sa empiric proton-pump-inhibitor treatment.
- EGD escalation: Isaalang-alang ang agarang endoscopic evaluation para sa alarm features (halimbawa dysphagia/odynophagia, anemia/low red-cell indices, hematemesis, o unintended weight loss) at para masuri ang erosive injury, Barrett change, stricture, o malignancy risk.
- Biopsy confirmation for Barrett change: Kinukumpirma ng endoscopic tissue sampling ang intestinal metaplasia; nakatutulong sa surveillance planning ang segment length reporting (short vs long segment).
- Ambulatory reflux monitoring: Maaaring kailanganin sa refractory symptoms ang catheter-based LES-adjacent acid monitoring upang iugnay ang sintomas sa acid exposure.
Nursing Interventions
- Patibayin ang individualized risk-factor reduction at symptom-trigger avoidance strategies.
- Suportahan ang escalation ng diagnostics at treatment kapag nagpapatuloy ang sintomas o may lumilitaw na warning features.
- Itaguyod ang adherence sa long-term management plans na nagpapababa ng recurrence at injury progression.
- Iayon ang care plans sa pain reduction, pag-unawa sa lifestyle modification, healthy-weight progression, nutrition adequacy, at medication-adherence goals.
- Unahin ang lifestyle-first management: iwasang kumain sa loob ng humigit-kumulang 3 oras bago matulog, itaas ang ulunan ng kama ng humigit-kumulang 6-9 inches, at bawasan ang karaniwang trigger foods/beverages (halimbawa caffeine, chocolate, high-citrus, heavily spiced, o carbonated items).
- Suportahan ang weight-reduction planning kapag nakadadagdag ang obesity sa reflux burden.
- Hikayatin ang small, frequent meals at upright positioning habang/pagkatapos kumain upang mabawasan ang reflux burden.
- Para sa refractory disease o hindi matanggap na medication effects, ihanda ang mga kliyente sa surgical pathways gaya ng laparoscopic Nissen fundoplication, lalo na kung may malaking hiatal hernia.
- I-monitor ang postoperative symptom changes pagkatapos ng fundoplication, kabilang ang transient bloating, dysphagia, at nabawasang kakayahang mag-burp, habang tinitingnan ang kabuuang pagbuti ng reflux.
- Turuan ang warning monitoring para sa posibleng erosive bleeding (dugo sa suka o dumi) at patibayin ang smoking cessation, alcohol avoidance, at pagbawas ng pressure-raising behaviors (straining, madalas na pagyuko, forceful coughing).
Pharmacology
| Drug Class | Role in GERD Care | Key Nursing Considerations |
|---|---|---|
| proton-pump-inhibitors (PPIs and H2 blockers) | First-line acid suppression kapag hindi sapat ang lifestyle measures | Karaniwang mas pinipili ang PPIs para sa nonerosive at erosive disease control; patibayin ang adherence at monitoring plan. |
| proton-pump-inhibitors (H2 receptor antagonists) | Karagdagang acid suppression option sa piling symptom patterns | May OTC at prescription pathways; beripikahin ang self-medication use at tugon. |
| antiemetics (prokinetic therapy) | Motility support sa piling refractory patterns | Maaaring malimitahan ang metoclopramide use ng long-term adverse-effect risk, kaya mahalaga ang benefit-risk reassessment. |
Related Concepts
- proton-pump-inhibitors - First-line acid suppression para sa maraming GERD presentations.
- digestive-system - Foundational esophageal at gastric physiology na kaugnay ng reflux.
- comprehensive-abdominal-assessment - Structured symptom at red-flag assessment.