Vital Sign Indicators of Physiologic Functioning at Homeostasis
Mahahalagang Punto
- Ang vital signs ay interdependent markers ng physiologic balance at early deterioration.
- Dapat pagsamahin sa interpretation ang normal ranges, age variation, baseline trend, at current context.
- Karaniwang sinusuri ang pain kasama ng vital signs dahil maaari nitong baguhin ang heart rate, respiratory pattern, at blood pressure.
- Dapat i-recheck at i-validate ng nurses ang unexpected readings bago kumilos batay sa iisang abnormal value.
- Sinusuportahan ng early-warning frameworks (halimbawa MEWS na may consciousness scoring) ang napapanahong escalation decisions.
- Nagbibigay ang pinagsamang vital-sign patterns ng praktikal na snapshot ng circulatory, respiratory, at neurologic status.
- Sa older adults, maaaring mas mababa ang baseline temperature, kaya maaaring clinically important infection pa rin ang high-normal readings.
Pisyopatolohiya
Ang homeostasis ay self-regulation process ng katawan sa temperature control, oxygenation, circulation, at ventilation. Ang vital signs ay bedside indicators kung stable o nanganganib ang regulasyong ito. Tuloy-tuloy na hinuhubog ng central autonomic control (kabilang ang medulla-oblongata pathways) at peripheral chemo/baroreceptor feedback loops (halimbawa carotid at renal pathways) ang vital-sign trends na ito.
Ang pagbabago sa isang vital sign ay maaaring magdulot ng compensatory changes sa iba. Halimbawa, maaaring tumaas ang pulse at blood pressure dahil sa pain o anxiety, habang maaaring tumaas ang respiratory effort at heart rate dahil sa hypoxemia bago lumitaw ang late desaturation. Ang hypoxemia ay tumutukoy sa reduced oxygen sa arterial blood, habang ang hypoxia ay tumutukoy sa inadequate oxygen delivery sa tissue level; maaaring magdulot ng ischemic injury sa oxygen-sensitive organs ang matagal na deficits. Dahil hindi specific sa pain ang abnormal vital signs, dapat ipares ang interpretation sa subjective report at behavioral findings; sinusuportahan ng post-intervention normalization ang analgesic effect ngunit hindi nito kinukumpirmang pain lang ang sanhi. Sa thermoregulation, pinapatakbo ng hypothalamic control ang vasodilation/sweating para sa heat loss at shivering para sa heat generation; dapat isaalang-alang ang circadian at metabolic variation bago i-label na pathologic ang minor temperature shifts.
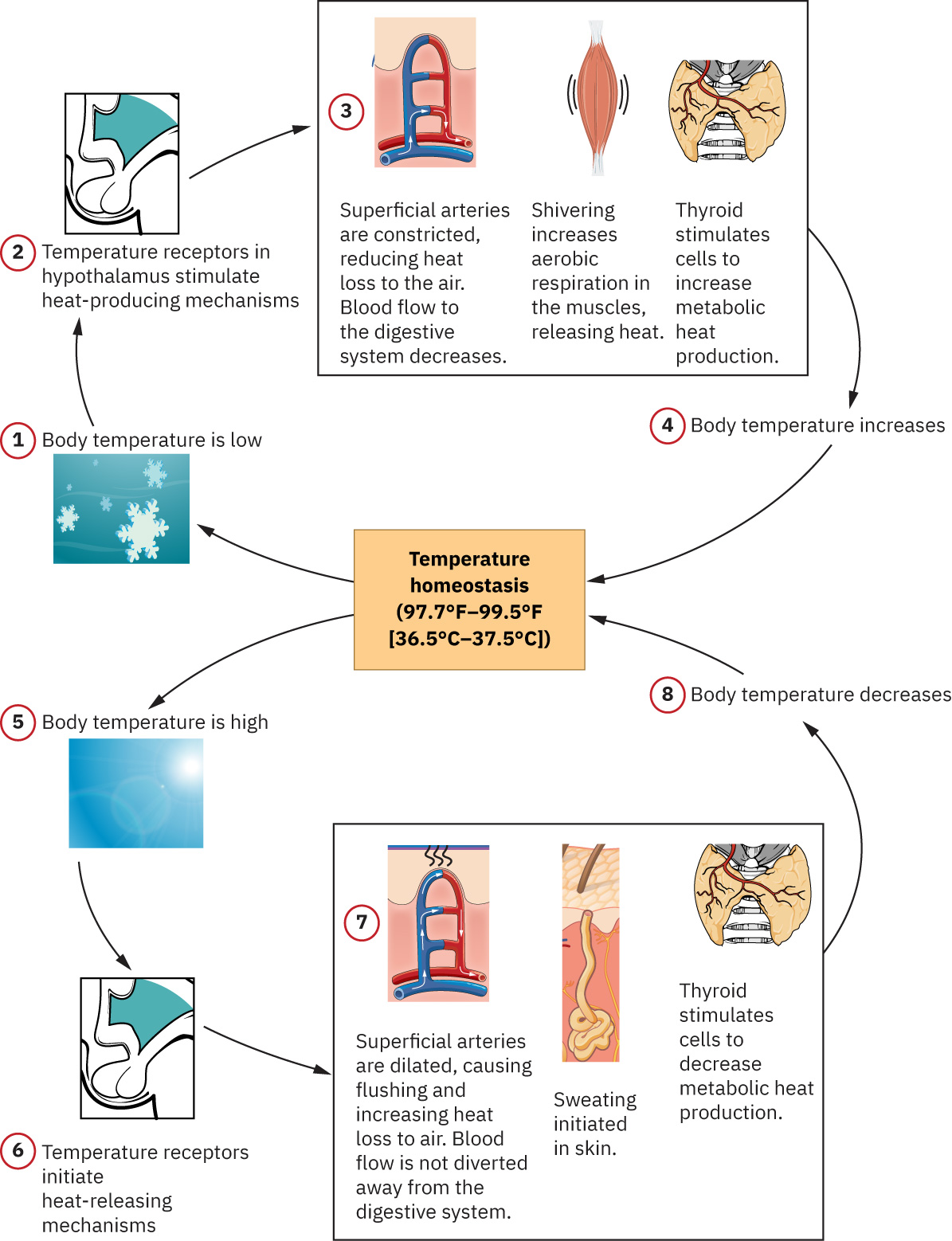 Illustration reference: OpenStax Fundamentals of Nursing Ch.7.1.
Illustration reference: OpenStax Fundamentals of Nursing Ch.7.1.
Dapat i-interpret ang severe temperature extremes bilang high-risk instability: ang core temperature na higit sa 105.8 F (41 C) ay nagpapahiwatig ng hyperthermia at mas mababa sa 95 F (35 C) ay nagpapahiwatig ng hypothermia, na madalas mula sa external exposure stressors at hindi routine circadian fluctuation.
Ang temperature na higit sa 100.4 F (38 C) ay pyrexia (fever); febrile ang patient na may fever, at afebrile status ang pagbabalik sa normal range.
Maaaring baguhin ng hormonal transitions (halimbawa menopause-related estrogen change) ang thermoregulatory sensitivity at perceived temperature instability.
Para sa pulse interpretation, ang cardiac output ay tinutukoy bilang CO = SV x HR (stroke volume times heart rate). Kapag malakas ang stroke volume (halimbawa trained athletes), maaaring mas mababa ang resting heart rate habang nananatiling sapat ang output. Sa kabilang dulo, maaaring bawasan ng severe tachycardia ang ventricular filling time, pababain ang stroke volume, at kalaunan ay pababain ang effective cardiac output kahit mabilis ang pulse.
Ipinapakita rin ng respiratory pattern ang acid-base compensation: madalas na nagtutulak ng tachypnea/hyperventilation ang nonpulmonary acidosis upang alisin ang CO2, habang maaaring magpakita ng hypoventilation/bradypnea ang nonpulmonary alkalosis.
Sinasalamin ng blood pressure trends ang interaction ng cardiac contractility, vascular tone/diameter, at circulating blood volume; dapat mag-trigger ng evaluation para sa shock physiology ang abrupt hypotension na may tachycardia.
Nagdaragdag ng perfusion context ang pulse pressure (systolic minus diastolic) at mean arterial pressure (MAP); pinapataas ng sustained MAP na mas mababa sa humigit-kumulang 60 mmHg ang ischemia risk mula sa inadequate tissue blood flow.
Nangyayari ang heat exchange sa kapaligiran sa apat na praktikal na pathways na nakaaapekto sa bedside temperature trends at comfort interventions:
- Conduction: Direct contact transfer (halimbawa ice packs, tepid sponge contact, cooling blankets), karaniwang maliit na bahagi ng total heat loss.
- Convection: Air o water current transfer (halimbawa fan, wind exposure, conditioned airflow), na maaaring pabilisin ang heat loss sa exposed patients.
- Radiation: Infrared-wave transfer na walang direct contact (halimbawa sun exposure, radiant warmers, room heat sources), madalas na pinakamalaking passive transfer component.
- Evaporation: Heat loss kapag nagiging vapor ang tubig (halimbawa perspiration), na malakas ang impluwensiya ng ambient humidity.
Klasipikasyon
- Thermoregulatory indicators: Temperature at fever/hypothermia patterns.
- Perfusion indicators: Pulse rate/rhythm/force at blood pressure trends.
- Ventilation and oxygenation indicators: Respiratory rate/quality at SpO2 trend.
- Integrated distress indicators: Pain at symptom context na nakaaapekto sa lahat ng domains.
- Consciousness-status indicators: AVPU/GCS-linked arousal at response trends na nagbabago ng deterioration risk.
- Escalation-score class: Pinagsasama ng Modified Early Warning Score (MEWS) ang vital signs at consciousness cues upang mag-trigger ng response tiering.
Pagsusuri sa Pag-aalaga
Pokus sa NCLEX
Binibigyang-diin ng priority decisions ang trend interpretation at immediate verification ng unexpected abnormalities.
- Suriin ang bawat vital sign gamit ang route/method accuracy at standardized timing.
- Gumamit ng contextual SpO2 targets: karamihan sa adults
94-98%; maaaring gumamit ng mas mababang ordered targets tulad ng88-92%ang selected chronic-hypercapnic profiles (halimbawa ilang COPD patients). - I-verify na angkop sa pasyente ang equipment size at configuration (lalo na BP cuff sizing at sensor fit).
- Suriin ang prior trends, clinical history, at ordered monitoring parameters bago mag-interpret.
- Ihambing ang findings sa age-specific ranges at patient baseline.
- Sa pediatric workflows, asahan ang routine blood-pressure screening mula humigit-kumulang edad 3 (mas maaga kung may cardiac-risk concerns) at i-interpret ang pediatric BP ayon sa age, height, at sex-specific norms.
- Suriin ang context factors tulad ng activity, pain, anxiety, medications, at environment.
- Suriin ang required monitoring cadence ayon sa setting at acuity (halimbawa routine acute-care intervals, high-frequency critical-care surveillance, outpatient visit-based checks, o long-term-care daily/as-needed schedules).
- Suriin ang exposure risks na nagpapalala ng heat loss o gain (halimbawa inadequate clothing sa cold/windy settings, high ambient heat, prolonged wet skin).
- I-interpret ang pulse sa
rate,rhythm, atvolumecharacteristics, hindi sa rate lamang. - Suriin ang pulse equality sa pagitan ng sides kapag clinically indicated at iwasan ang simultaneous bilateral carotid palpation.
- Sa neonates, lalo na preterm infants, ituring ang low temperature na high risk dahil ang immature shivering response at limited brown-fat reserve ay nagpapababa ng heat-generation capacity.
- Para sa older adults, i-monitor ang mental-status change (confusion, disorientation, agitation) bilang posibleng temperature-related deterioration cue.
- Isaalang-alang ang menstrual-cycle timing, exercise load, at emotional arousal kapag ini-interpret ang mild temperature elevation.
- Iugnay ang pulse abnormalities sa mga malamang na physiologic drivers tulad ng fever/hyperthyroidism, hypoxemia, hypovolemia, structural heart failure, at electrical-conduction disorders.
- Igalang ang site/route limitations na dulot ng history (halimbawa post-mastectomy arm precautions, wound-related site exclusions, oral-route contraindications).
- Suriin ang concerning pattern combinations (halimbawa hypotension na may tachycardia).
- I-track ang respiratory pattern quality (rate, rhythm, depth) at tukuyin ang high-risk abnormalities tulad ng apnea episodes, Kussmaul pattern, o Cheyne-Stokes cycles.
- Sa newborns at infants, bilangin ang respirations sa buong isang minuto habang kalmado; karaniwang nasa humigit-kumulang
30-60/minang newborn respiratory rate at nagbabago ayon sa sleep-wake state. - Sa infants na obligate nose breathers, suriin ang nasal patency dahil maaaring mabilis lumala ang respiratory distress dahil sa congestion o occlusion.
- Ituring ang dyspnea na may accessory-muscle use, tripod posture, o orthopnea bilang escalation cues para sa posibleng respiratory o cardiopulmonary decompensation.
- Gumamit ng pediatric oxygen-saturation expectations na humigit-kumulang
95-100%sa karamihan ng children maliban kung may partikular na alternate target na naka-order. - Suriin kung technical artifact ang isang reading at nangangailangan ng repeat measurement.
- Kilalanin ang pulse-oximetry limitations sa severe anemia, reduced peripheral perfusion, at dyshemoglobinemia exposure contexts (halimbawa carbon monoxide), at i-escalate sa confirmatory testing kapag hindi tugma ang readings at presentation.
- Kapag available, kalkulahin at i-trend ang MEWS sa bawat set ng abnormal vital signs o neurologic concern.
- Isama ang level-of-consciousness findings (A&O status, AVPU, o GCS) sa physiologic readings sa halip na i-interpret ang vitals nang hiwa-hiwalay.
Mga Interbensyon sa Pag-aalaga
- I-recheck ang abnormal values gamit ang tamang technique at alternate method/site kapag kailangan.
- I-validate sa manual assessment ang electronically monitored values kapag hindi tugma ang readings sa clinical presentation.
- I-escalate agad ang validated high-risk changes ayon sa facility protocol.
- Unahin ang urgent assessment para sa unexpectedly low temperatures sa infection-risk patients, lalo na sa age extremes.
- I-dokumento nang malinaw ang value, method, context, at follow-up action.
- I-coordinate ang symptom at cause-directed interventions sa halip na isolated number treatment.
- Turuan ang patients tungkol sa expected ranges, warning signs, at kung kailan dapat i-notify ang providers.
- Ituring ang ordered cadence bilang minimum; kumuha ng karagdagang full vital-sign set kapag may pagbabago sa status o concern mula sa patient/family/team.
- Kapag delegated ang collection, i-verify ang data quality at panatilihin ang RN accountability para sa interpretation at escalation decisions.
- Kung pinaghihinalaan ang device malfunction, alisin sa paggamit ang equipment, lagyan ng tamang label, at i-route para sa technical/biomed evaluation.
- Gamitin ang tiered MEWS response bilang practical guide kapag lokal na inadopt:
0-1: routine monitoring2-3: dagdagan ang monitoring frequency (madalas q2h) at isaalang-alang ang provider communication kung persistent4-6: i-notify ang provider at dagdagan ang monitoring (madalas hourly)>=7: i-activate ang rapid response/emergency pathway ayon sa policy
Single-Reading Error
Ang pagkilos batay sa isang unvalidated outlier ay maaaring magpaantala sa angkop na care o mag-trigger ng hindi kailangang intervention.
Parmakolohiya
Maraming medications ang nakaaapekto sa vital signs (halimbawa beta blockers na nakaaapekto sa pulse at blood pressure). Dapat isama sa trend interpretation ang kasalukuyang pharmacologic profile bago magkonklusyon ng deterioration.
Paglalapat ng Klinikal na Paghuhusga
Klinikal na Sitwasyon
Ang pasyente ay may bagong shortness of breath, maputlang balat, tachycardia, at mas mababang blood pressure kaysa baseline.
- Recognize Cues: Ipinapahiwatig ng maraming magkakaugnay na vital-sign changes ang instability.
- Analyze Cues: Ipinapakita ng findings ang posibleng perfusion at oxygenation compromise.
- Prioritize Hypotheses: Agarang prayoridad ang pag-validate ng readings at pagpigil ng deterioration.
- Generate Solutions: Ulitin ang vitals, muling suriin ang respiratory effort, at mag-escalate nang mabilis.
- Take Action: I-notify ang provider/rapid response ayon sa protocol at simulan ang supportive care.
- Evaluate Outcomes: Kinukumpirma ng stabilizing trend ang intervention effectiveness.
Mga Kaugnay na Konsepto
- pagsukat ng body temperature sa maraming routes - Nakaaapekto ang route selection at technique sa temperature validity.
- pagsukat ng radial pulse - Sumusuporta ang pulse rate at rhythm trends sa perfusion analysis.
- pagsukat ng respirations - Nagbibigay ng early compromise cues ang respiratory quality at rate.
- pagsukat ng blood pressure: manual at automatic methods - Mahalaga ang accurate cuff method para sa perfusion decisions.
- pagsukat ng oxygen saturation gamit ang pulse oximetry - Nangangailangan ng artifact awareness ang SpO2 interpretation.
Sariling Pagsusuri
- Bakit dapat i-interpret ng nurses ang vital signs bilang pattern at hindi isolated values?
- Aling factors ang maaaring lumikha ng false abnormal reading na nangangailangan ng recheck?
- Paano mababago ng pain ang hindi bababa sa tatlong ibang vital sign indicators?