Subcutaneous Medication Administration
Key Points
- Subcutaneous (SQ) injections deliver medication into fatty tissue for slower, sustained absorption.
- Common sites include abdomen, upper arms, thighs, and buttocks; abdomen is often preferred.
- Technique safety depends on aseptic preparation, correct needle selection, and angle/body-size matching.
- Needle length should be individualized for tissue depth, including shorter choices in very thin/cachectic patients.
- Some ordered SQ medications may be delivered via prefilled pen or auto-injector devices using product-specific activation steps.
- SQ absorption can change with local blood-flow shifts (for example strenuous exercise or local heat/cold exposure at the site).
- Typical SQ doses are often up to about 1 mL per injection in many adults; infants and small children commonly use smaller volumes (often up to about 0.5 mL) unless policy/order specifies otherwise.
Equipment
- Ordered SQ medication and syringe
- Needle typically 25G-31G and 3/8 to 5/8 in (9.5 to 15.9 mm), adjusted by age/body habitus and site
- Needleless injector option when medication/device policy supports SQ administration
- Antiseptic solution and gloves
- Sharps container and documentation tools
Procedure Steps
- Verify patient identity, order, and medication rights before preparation.
- Assess suitability for SQ route, including tissue thickness, medication volume, and patient factors (including cachexia/thin habitus that may require shorter needle selection), and verify ordered volume aligns with site-specific tolerance.
- Select site (abdomen, upper arm, anterior thigh, upper ventral gluteal region, or upper back) and inspect skin integrity; for abdominal use, stay at least about 2 in (5 cm) from the umbilicus.
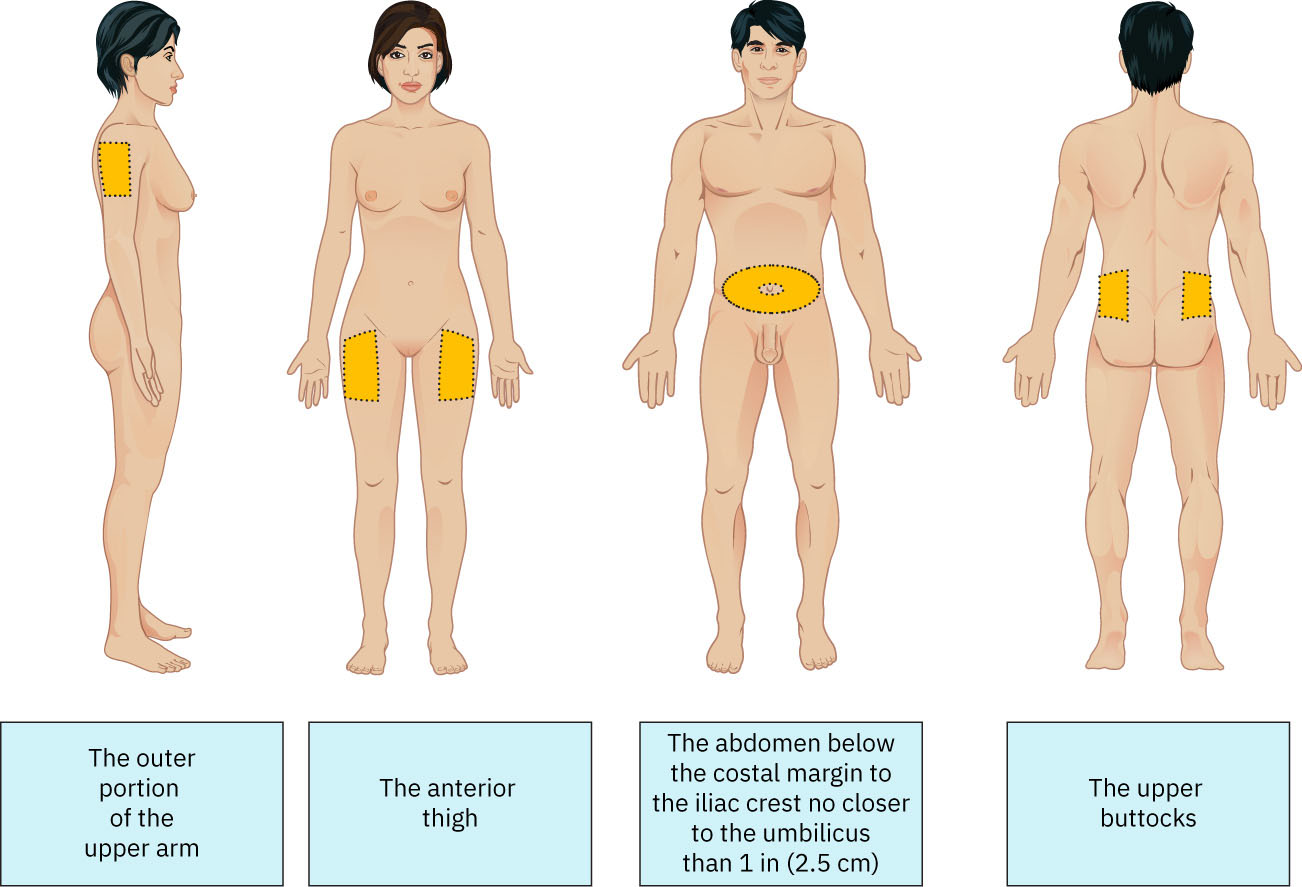 Illustration reference: OpenStax Fundamentals of Nursing Ch.11.3.
Illustration reference: OpenStax Fundamentals of Nursing Ch.11.3. - Avoid sites that are bruised, scarred, open, over bony prominences, or affected by local infection/inflammation (for example cellulitis) or impaired tissue perfusion.
- Perform hand hygiene, apply nonsterile gloves, and if skin is visibly soiled cleanse with soap and water first; then prep with alcohol swab in a center-out circular motion (about 2 in/5 cm radius) for about 30 seconds and allow to dry.
- Prepare medication and pinch skin to create a skinfold.
- Insert needle with a quick, dart-like motion at a 45- to 90-degree angle based on tissue depth/body size; 90 degrees is common for normal/obese adults, and 45 degrees is commonly used when tissue is thin or skinfold depth is limited.
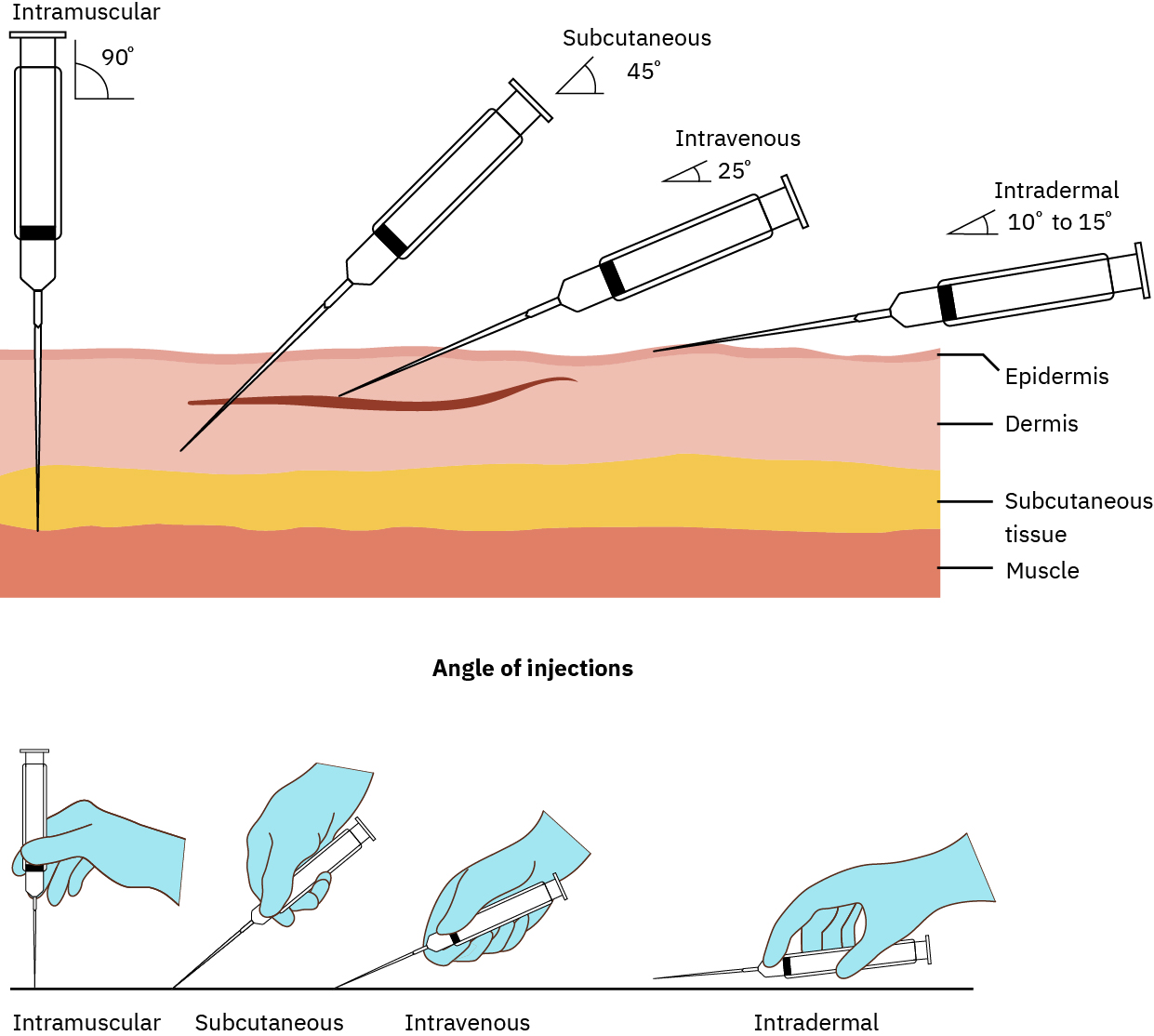 Illustration reference: OpenStax Clinical Nursing Skills Ch.12.
Illustration reference: OpenStax Clinical Nursing Skills Ch.12. - Inject medication slowly (about 10 seconds per mL when tolerated); routine aspiration is not required for SQ injections.
- After completing medication delivery, hold the needle in place for about 10 seconds when indicated by product/protocol (for example many insulin-pen workflows) before withdrawal.
- Withdraw needle at the same angle used for insertion and apply gentle pressure with sterile gauze.
- Engage needle safety device immediately after injection (prefer hard-surface activation rather than finger activation when applicable), avoid recapping, and dispose needle and syringe in puncture-proof sharps container.
- Do not massage the site after injection.
- Document route, dose, site, and patient response/adverse reactions.
- Rotate sites systematically to reduce lipoatrophy and lipohypertrophy risk.
Medication-Specific Considerations
Heparin (SQ): high-alert medication requiring independent double-check of product, concentration, and dose; review coagulation parameters (for example PTT/aPTT per protocol), and for LMWH/heparin exposure follow platelet monitoring per policy for thrombocytopenia risk. Rotate injection sites, prefer abdominal tissue at least about 2 in (5 cm) from umbilicus, inject at 90 degrees over about 30 seconds, maintain skinfold when indicated, and do not massage after injection to reduce hematoma risk.Insulin (SQ): high-alert medication requiring independent double-check of insulin type and dose before preparation and again before administration; use insulin syringes calibrated in units, verify product integrity (not expired and no unexpected discoloration/clumping), and time doses with meals/acting profile and current glucose results per policy. For insulin pens, use a new needle for each injection, prime per manufacturer guidance (commonly about 2 units), keep the pen in place about 10 seconds after injection, and never share pens between patients.Age-site anchor (vaccine-focused SQ use): birth to 12 months commonly uses fatty tissue over the anterolateral thigh, while 12 months and older commonly uses fatty tissue over the triceps.
Common Errors
- Poor site/angle selection → unreliable absorption and tissue trauma risk.
- Breaks in aseptic technique → injection-site infection risk.
- Rapid forceful injection → increased discomfort and local tissue injury.
- Inadequate skin prep contact/dry time → contamination and local irritation risk.
- Exceeding site-specific SQ volume tolerance → leakage, poor absorption, and injection-site pain risk.
- Using bruised/tender/hard/swollen or bony-prominence sites → higher pain, tissue injury, and absorption variability risk.
- Puncturing through a skin fold during insertion → accidental needlestick and technique failure risk.
- Massaging site after SQ heparin → hematoma and bruising risk.
- Incomplete site documentation → unsafe rotation and continuity gaps.
Related
- intradermal-medication-administration - Distinguishes dermal versus subcutaneous depth and technique.
- oral-medication-administration-safety - Medication rights and post-administration evaluation principles apply across routes.