Intradermal Medication Administration
Key Points
- Intradermal injections deliver small medication volumes into the dermis for testing and selected medications.
- Limited dermal blood flow produces slower absorption and minimal systemic exposure for most ID indications.
- Typical ID injection volume is small (often about 0.1 mL for TB/allergy testing); larger therapeutic ID doses are limited by policy because excess volume increases leakage and interpretation error risk.
- Correct technique uses a shallow insertion angle (commonly about 5-15 degrees) with small-gauge needle selection.
- Formation of a wheal/bleb indicates appropriate intradermal placement.
- Common ID uses include tuberculosis testing, allergy testing, local anesthetic testing/administration, selected lesion-directed steroid injections, and some botulinum toxin protocols.
- For Mantoux TST, interpretation is based on induration (not erythema), measured in millimeters within the required read window.
- ID technique uses bevel-up shallow insertion, does not require aspiration, and avoids post-injection massage to prevent spread into deeper tissue.
Equipment
- Ordered intradermal medication and syringe
- Needle typically 25 to 27 gauge and 3/8 to 5/8 in (9.5 to 15.9 mm)
- Antiseptic solution, gauze, and optional adhesive dressing
- Documentation tool for route, site, dose, and response
Procedure Steps
- Verify patient identity, order, and medication rights before preparation, including that ordered ID volume is within route limit (typically ⇐ 0.5 mL).
- Select an appropriate site (for example inner/anterior forearm, posterior upper arm, upper back under scapula, or upper chest) according to test/medication protocol.
- Assess skin integrity and prior adverse intradermal reaction history; avoid sites with lesions, rash, moles, scars, sores, or prominent veins. For intralesional steroids, avoid active infection sites and known steroid-allergy contexts.
- If skin is visibly soiled, cleanse with soap and water first; then cleanse with alcohol swab in a center-out circular motion (about 2 in/5 cm radius) for about 30 seconds and allow to dry.
- Insert needle bevel-up at a shallow angle (commonly about 5-15 degrees), advancing only enough to cover the bevel (commonly no more than about 1/8 in) into the dermis.
- Inject medication slowly to minimize tissue trauma and leakage; routine aspiration is not required for ID technique.
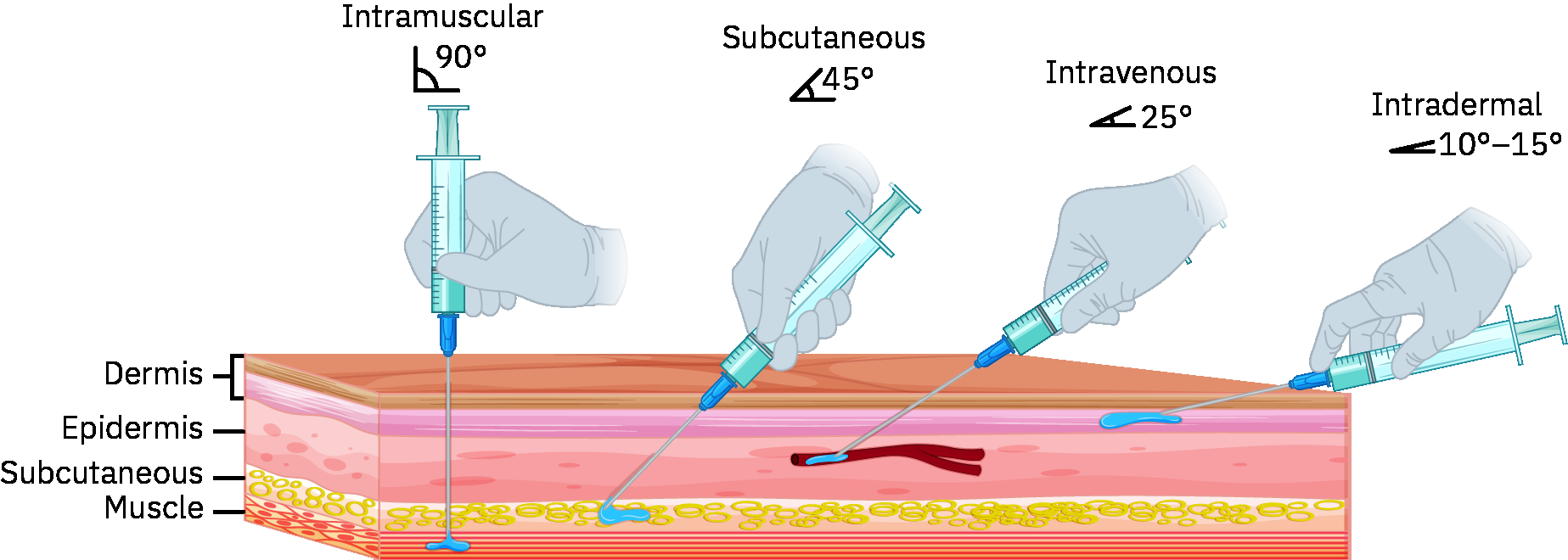 Illustration reference: OpenStax Pharmacology Ch.2.3.
Illustration reference: OpenStax Pharmacology Ch.2.3. - Confirm wheal/bleb formation, indicating correct placement.
- For multi-allergen testing, label or map each site clearly to preserve correct allergen-result interpretation.
- Withdraw needle at the same angle as insertion, engage safety device without recapping when available, and avoid massaging or occlusive covering of skin-test sites; use gentle gauze only if minor bleeding is present.
- Monitor site for localized redness/wheal and systemic reactions (for example generalized rash, respiratory symptoms, or anaphylaxis) according to protocol.
- Ensure immediate access to emergency allergy-response medications/equipment when performing allergen testing.
- For tuberculin skin testing, schedule/perform read at 48-72 hours and repeat testing per policy if the read window is missed.
- For TST interpretation, assess and measure induration diameter in millimeters (not erythema) and record 0 mm when no induration is present.
- Do not massage the site after injection.
- Teach patient to avoid scratching or rubbing the site.
- Document medication, dose, route, site mapping when applicable, TB measurement details when applicable, and patient response.
Common Errors
- Incorrect injection angle or depth → failed intradermal placement and invalid test result.
- Not confirming wheal/bleb → uncertain medication deposition.
- Rubbing/scratching the site → irritation and inaccurate skin-test interpretation.
- Missing site labeling during multi-allergen testing → interpretation and treatment errors.
- Performing allergy testing without emergency-response readiness → delayed treatment of severe reactions.
- Reading TST by redness instead of induration or outside the read window → invalid TB-screen interpretation risk.
- Massaging site after ID injection → unintended spread into subcutaneous tissue and distorted response.
- Incomplete documentation → unsafe continuity and interpretation gaps.
Related
- oral-medication-administration-safety - Route-specific safety checks align with shared medication-rights workflow.
- medication-rights-and-three-checkpoint-verification - Comprehensive framework for nursing assessment, documentation, and evaluation responsibilities.