Intramuscular Medication Administration
Key Points
- Intramuscular (IM) injections deliver medication into muscle tissue with generally faster absorption than SQ routes because of richer muscle blood supply.
- IM route is commonly preferred over SQ when larger medication volumes are required.
- Common sites include deltoid, vastus lateralis, and ventrogluteal regions.
- Avoid routine dorsogluteal use unless specifically indicated because of higher sciatic nerve injury risk.
- IM absorption rate varies with site blood supply; higher-perfusion muscle beds absorb faster.
- Correct technique uses a 90-degree insertion angle with age/body-size appropriate needle selection.
- Needle length should be adjusted for body habitus, including shorter selections in very thin/cachectic patients when depth permits safe muscle deposition.
- Pediatric IM administration requires age/size-specific site and needle decisions (for example shorter needles and smaller gauges in infants/small children, with vastus lateralis commonly preferred).
- IM maximum volume depends on site and age; confirm local policy limits before mixing or administering larger-volume doses.
- Common baseline volume anchors are about 0.5-1 mL for infants/small children and about 2-3 mL for many adults, then refine by site, medication, and policy.
- Older adults and very thin/cachectic patients may tolerate lower single-site volumes (commonly around 2 mL) even when larger adult limits exist.
- Major IM complications from poor technique include pain, abscess/cellulitis, bone or nerve injury, and local muscle damage/atrophy.
Equipment
- Ordered IM medication and syringe
- Needle typically 5/8 to 1.5 in (15.9 to 38.1 mm), selected by body habitus and site depth
- Gauge by medication type: aqueous 20G-25G, oil-based/viscous 18G-21G, many immunizations 22G-25G (smaller pediatric gauges such as 25G-27G may be selected when clinically appropriate)
- Needleless injector option when medication/device policy supports IM administration
- Antiseptic solution, gloves, and sterile supplies
- Sharps container and documentation tools
Procedure Steps
- Verify patient identity, medication order, and medication rights.
- Assess patient suitability for IM route, including muscle mass, adipose thickness, injection volume, medication factors, and body-habitus factors (for example cachexia) that may require needle-length adjustment; in pediatric patients, include developmental stage, BMI, and muscle tone in site/needle planning; verify planned volume is within site/age limits.
- Select appropriate site based on age and condition (for vaccine-focused pediatric use, vastus lateralis is commonly preferred through about age 3 years, with deltoid commonly preferred at age 3 years and older when muscle mass is adequate; ventrogluteal/deltoid/vastus lateralis remain core options by indication).
- Confirm selected site is free of pain, infection, abrasion, necrosis, marked atrophy, and clinically significant local perfusion compromise; rotate repeated IM sites to reduce hypertrophy and tissue injury.
- Perform hand hygiene; if skin is visibly soiled, cleanse with soap and water first, then prep with alcohol swab in a center-out circular motion (about 2 in/5 cm radius) for about 15 seconds and allow to dry about 30 seconds.
- Prepare medication and select proper needle gauge/length for patient age and body composition.
- If medication is drawn from a vial, replace the draw-up needle with a new injection needle before administration.
- Insert needle with quick dart-like motion at 90 degrees into target muscle (bevel up), stabilizing tissue/muscle as needed.
- Aspirate only when indicated by policy/medication context; if blood return appears, discard dose and restart with new medication/supplies.
- Inject medication slowly (about 10 seconds per mL unless otherwise specified), leave the needle in place for about 10 seconds after full delivery when tolerated, then withdraw at the same angle; apply gentle sterile gauze pressure and avoid forceful rubbing unless medication-specific guidance indicates massage.
- Engage needle safety device immediately after injection (prefer hard-surface activation rather than finger activation when applicable), avoid recapping, and dispose needle/syringe in puncture-proof sharps container.
- Document medication, dose, route, site, needle details when relevant, and patient response/adverse reactions.
Site Landmark Notes
Deltoid: inject in the central deltoid mass about 1-2 in (2.5-5 cm) below acromion. A practical landmark method is about three finger breadths below acromion to reduce subcutaneous, nerve, or joint injury risk. Deltoid single-injection volume is generally limited to about 1 mL in many adult protocols unless policy/order specifies otherwise.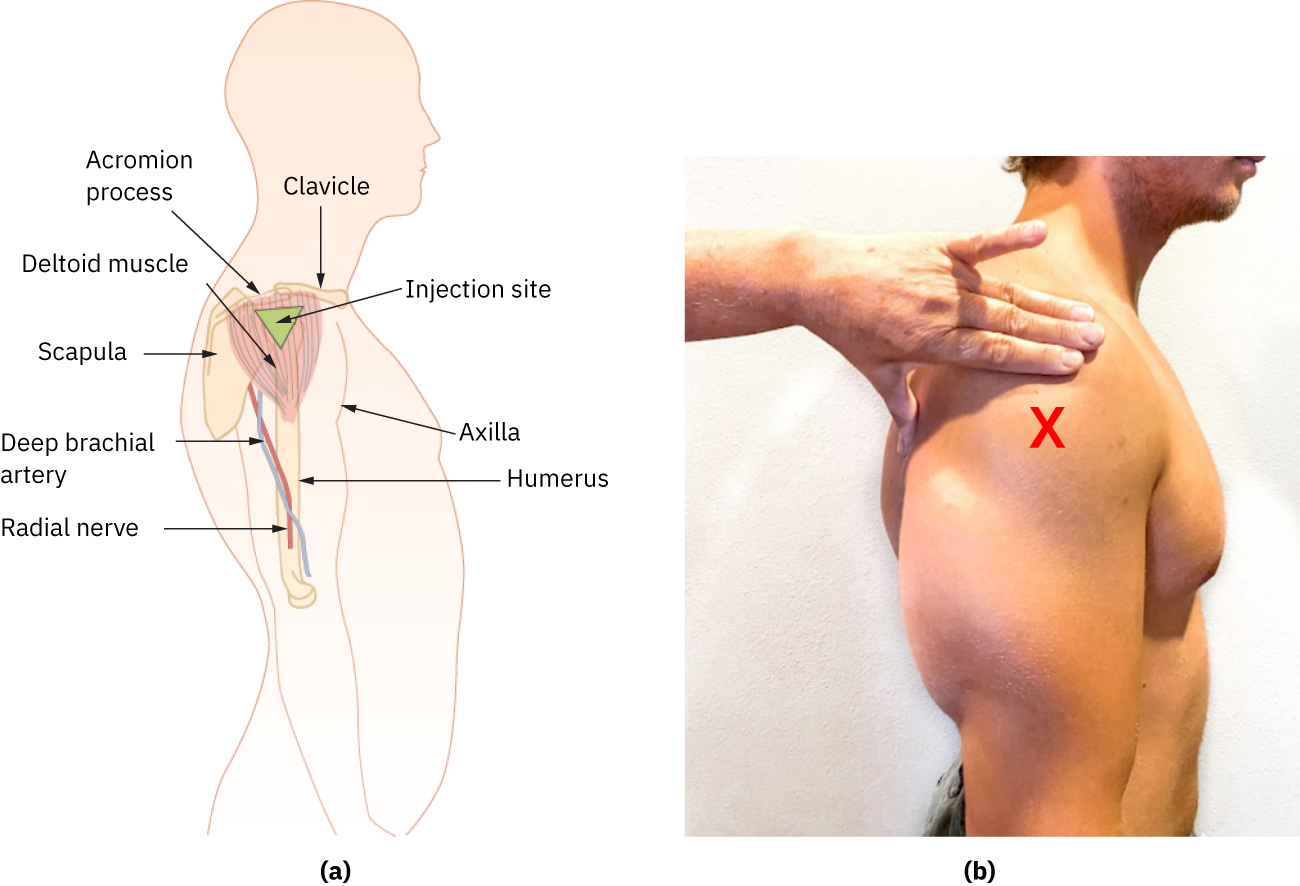 Illustration reference: OpenStax Clinical Nursing Skills Ch.12.
Illustration reference: OpenStax Clinical Nursing Skills Ch.12.Vastus lateralis: use the anterolateral thigh region from about one hand breadth above the knee to one hand breadth below the greater trochanter; preferred IM site in infants/toddlers and commonly used in broader pediatric pathways because of muscle development. Typical site-volume anchor is up to about 3 mL in many adults, with lower limits in children per policy.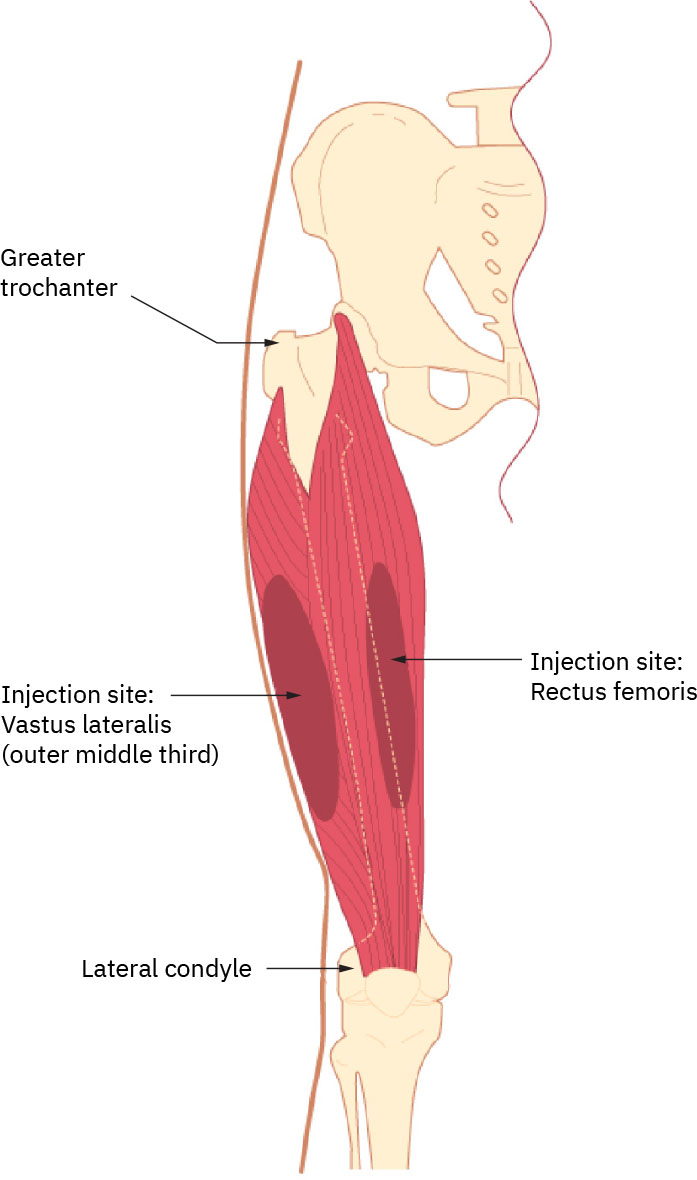 Illustration reference: OpenStax Clinical Nursing Skills Ch.12.
Illustration reference: OpenStax Clinical Nursing Skills Ch.12.Ventrogluteal: considered one of the safest IM sites in children and adults because of thick muscle and lower major nerve/vessel risk; preferred for many irritating or oil-based IM medications. With patient supine or side-lying, place palm on greater trochanter (opposite hand to hip), index finger toward anterior superior iliac spine, and middle finger along iliac crest to form a V, then inject in the center of the V. Typical site-volume anchors are up to about 3 mL in many adults and up to about 1 mL in children unless policy/order specifies otherwise.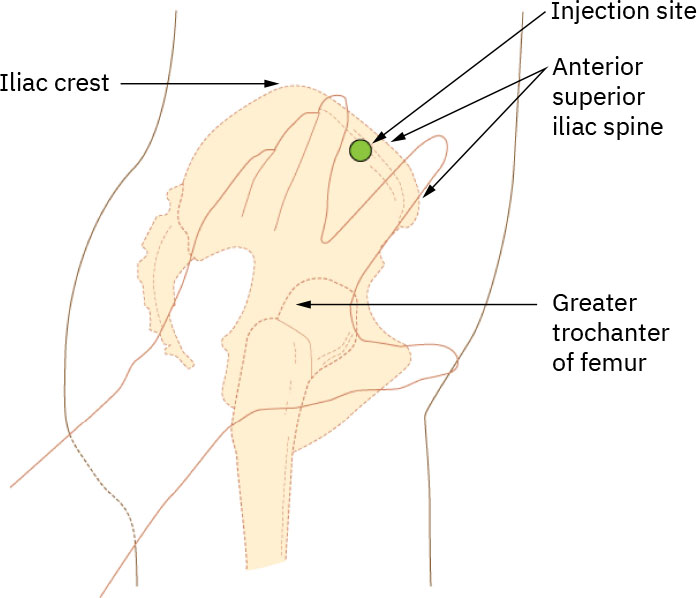 Illustration reference: OpenStax Clinical Nursing Skills Ch.12.
Illustration reference: OpenStax Clinical Nursing Skills Ch.12.Dorsogluteal: avoid routine use because of higher sciatic injury risk; use only when specifically indicated by policy/order and landmark carefully.Vaccine-age needle anchor: Newborns often use anterolateral thigh with about 5/8 in needle (22G-25G); infants commonly about 1 in (22G-25G); toddlers about 1-1 1/4 in thigh or 5/8-1 in deltoid if adequate muscle; ages 3-10 years commonly deltoid 5/8-1 in (22G-25G); ages 11+ commonly deltoid 5/8-1 in (22G-25G) with thigh alternatives by body size.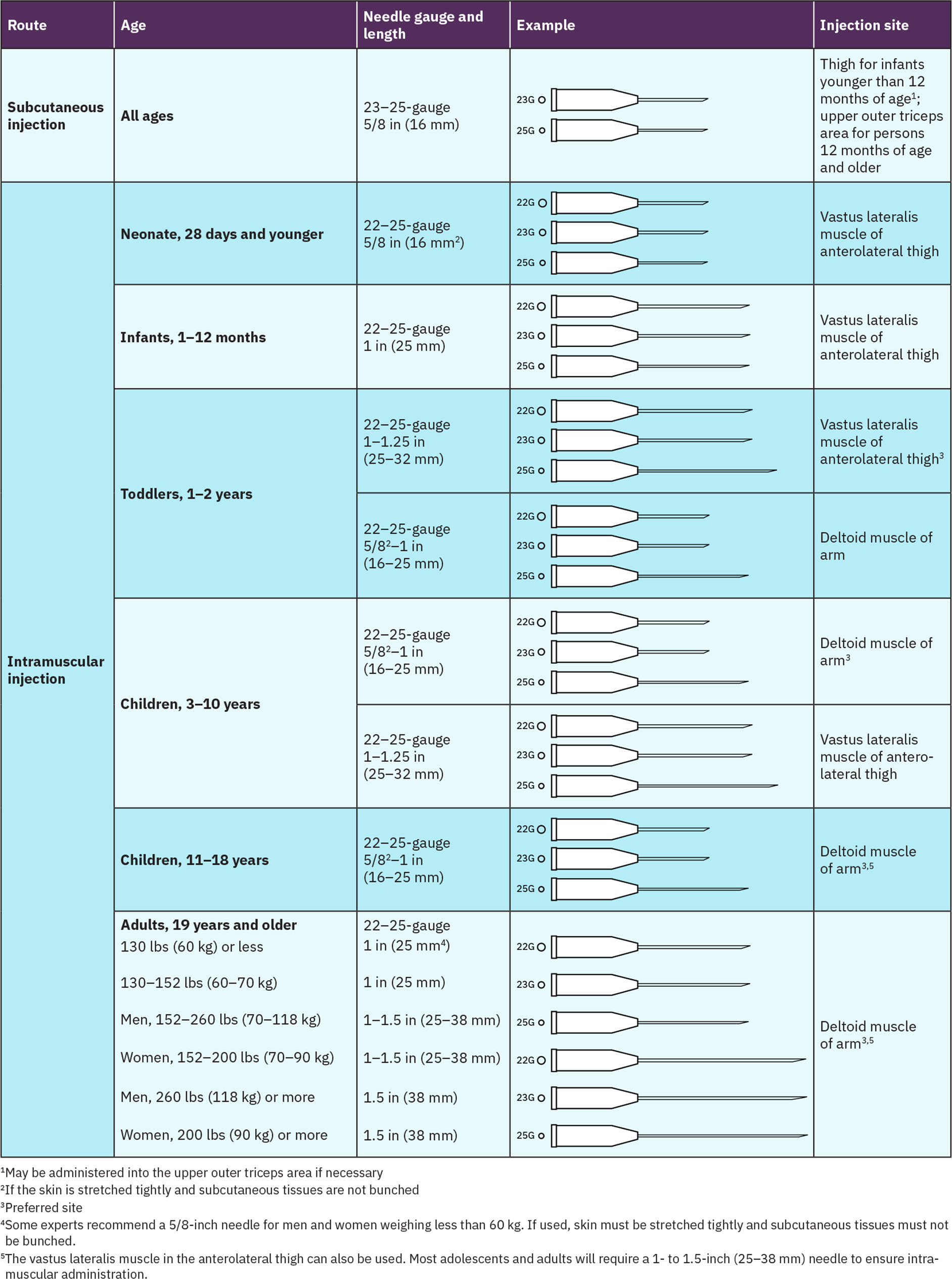 Illustration reference: OpenStax Clinical Nursing Skills Ch.12.
Illustration reference: OpenStax Clinical Nursing Skills Ch.12.
Technique Variations and Safety
Vaccinations: do not aspirate at recommended deltoid/vastus sites; if multiple vaccines are given, separate sites by about 1 in (2.5 cm) when feasible.Z-track: displace skin laterally/downward about 1 in (2.5 cm), inject while maintaining displacement, wait about 10 seconds before withdrawal, then release skin to seal track.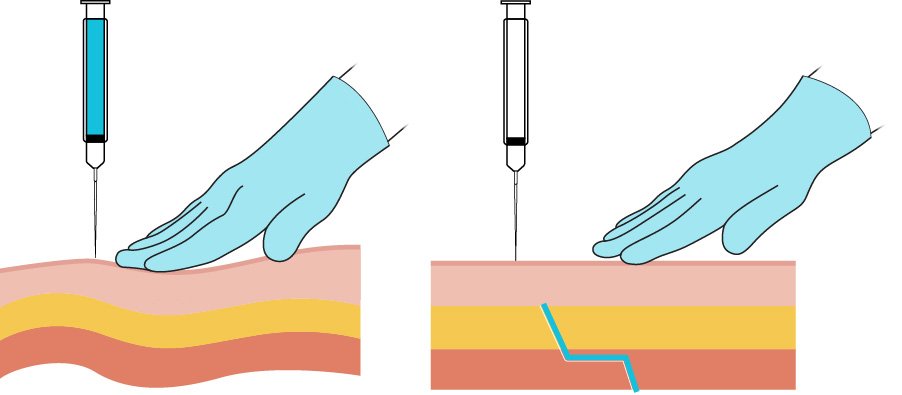 Illustration reference: OpenStax Clinical Nursing Skills Ch.12.
Illustration reference: OpenStax Clinical Nursing Skills Ch.12.Oil-based injections: often require lower-gauge (larger-bore) needles (for example 18G-21G) and thoughtful site rotation to avoid painful nodules.Injection-site reaction monitoring: mild redness/swelling/warmth/itching can occur; urgent escalation is required for breathing difficulty, hives, facial swelling, severe pain, or systemic symptoms suggestive of anaphylaxis.
Common Errors
- Poor site selection for medication volume/body habitus → ineffective delivery and tissue injury risk.
- Incorrect angle or needle length → suboptimal muscle deposition.
- Breaks in aseptic technique → injection-site infection risk.
- Inadequate skin prep contact/dry time → higher contamination and stinging risk.
- Exceeding IM volume tolerance for selected site/age → pain, tissue injury, and poor absorption risk.
- Delayed sharps disposal or incomplete documentation → safety and continuity failures.
Related
- subcutaneous-medication-administration - Distinguishes SQ versus IM depth and angle parameters.
- oral-medication-administration-safety - Medication rights, monitoring, and documentation principles apply across routes.