Medication Rights and Three Checkpoint Verification
Key Points
- Five core rights are right patient, right drug, right route, right time, and right dose.
- Additional safety rights include right reason, right documentation, and right response.
- Expanded pre-administration checks include right history/assessment, right interaction screening, right education/information, and informed right of refusal handling.
- Core rights are verified at three checkpoints: obtaining, preparing, and bedside administration.
- BCMA supports rights verification and can generate high-risk alerts before administration.
- Three-checkpoint verification is treated as a standard-of-care expectation for each medication administration event.
- Right-time verification should use four-digit military notation on MAR/eMAR to avoid AM/PM ambiguity.
- Right-time administration generally follows facility timing windows (commonly about +/-30 to 60 minutes by policy), but time-critical medications require tighter interval adherence.
- Pre-injection assessment should include current condition/history review, allergy-reaction profile, baseline clinical/lab status (including renal/hepatic function when relevant), and patient medication understanding.
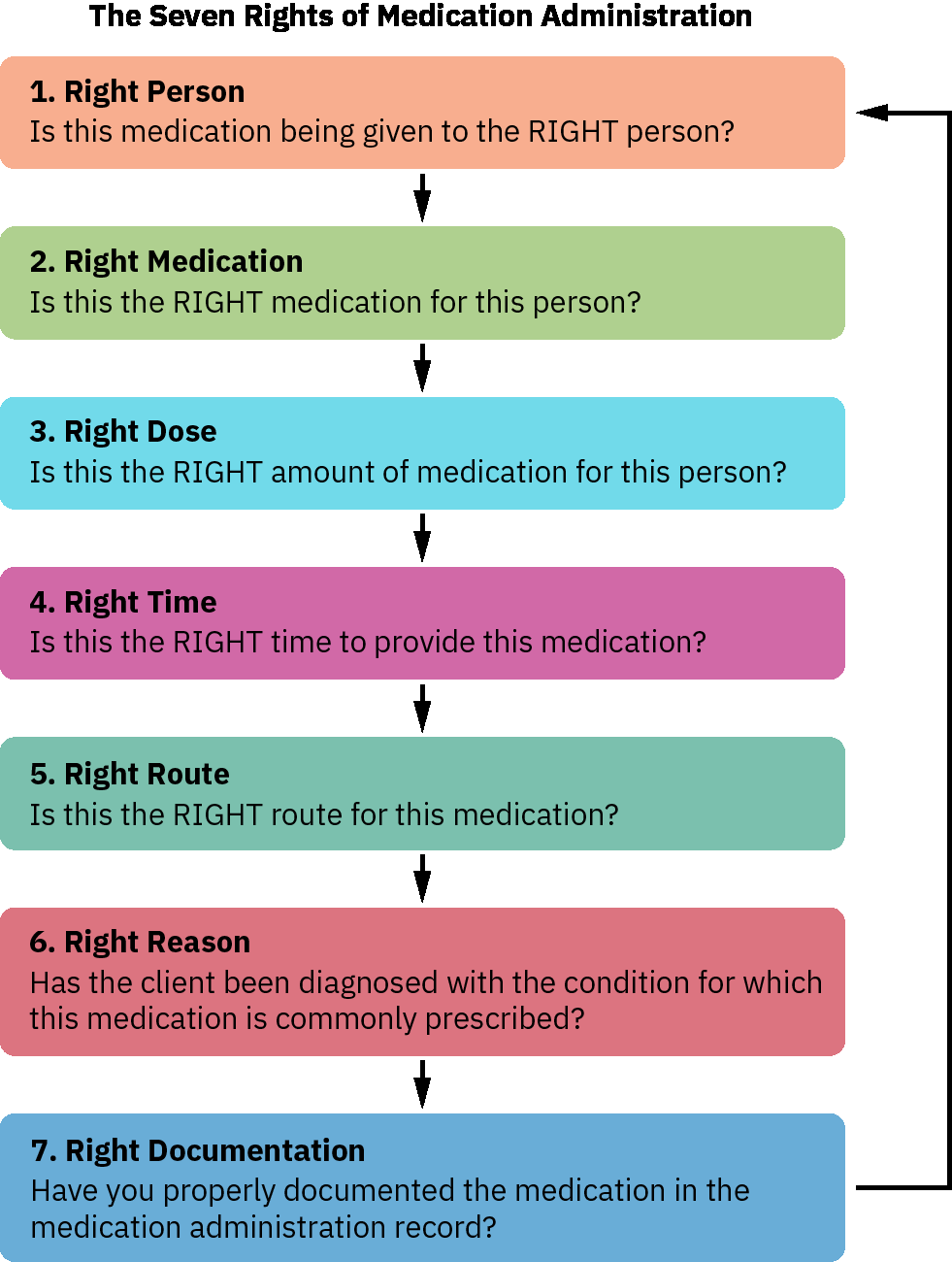 Illustration reference: OpenStax Pharmacology Ch.2.1.
Illustration reference: OpenStax Pharmacology Ch.2.1.
Equipment
- MAR and active medication order access
- Patient identifiers (armband and verbal confirmation when possible)
- Medication labels and dosage-calculation support
- BCMA scanner and workstation access
Procedure Steps
- Confirm right patient using at least two identifiers and never use room number as an identifier.
- Compare the MAR/eMAR against the active prescriber order for completeness and consistency before medication retrieval.
- At medication retrieval, compare label to order for right drug, right dose, right route, and right time.
- During preparation, repeat label-order comparison and verify expiration date and allergy status; if an allergy conflict exists, do not prepare/administer and notify the provider.
- At bedside, complete the third rights check before administration, including route feasibility; if route must change, obtain a new provider order before giving the medication.
- Confirm right time by checking prescribed frequency and when the last dose was administered, using MAR/eMAR four-digit military notation (for example 0700, 1900) rather than AM/PM wording.
- Apply facility medication-time policy windows (commonly about 30 to 60 minutes before/after scheduled time by policy) and prioritize exact interval timing for time-critical drugs (for example q8h antibiotics).
- Confirm right reason by linking medication mechanism to the current indication.
- Complete expanded safety checks: verify relevant history/assessment data (including current condition, past medical/medication history, pre-dose vital-sign and lab parameters such as renal/hepatic function when clinically relevant, and PRN indication baseline), review interaction risks (drug-drug, drug-food, drug-condition), review an evidence-based drug reference for onset/peak/action and key nursing considerations, provide medication education (expected therapeutic and adverse effects plus side-effect reporting instructions), and honor informed refusal workflow when applicable.
- For minors or capacity-limited patients, align medication-information sharing and consent/refusal pathways with governing law and organizational policy (for example parent/legal guardian notification requirements).
- Use BCMA scanning of patient armband and medication label to reinforce rights verification and review generated alerts (for example allergy flags, pre-dose vital-sign checks, and second-clinician verification prompts).
- Administer medication only when all rights checks are satisfied and no unresolved alert remains.
- Complete right documentation immediately after administration and record required details.
- Assess right response by evaluating if the desired effect occurred and document findings.
Common Errors
- Skipping one of the three checkpoints → increased wrong-patient or wrong-drug risk.
- Proceeding after unresolved BCMA or allergy alert → preventable adverse-event risk.
- Incomplete right-reason review → medication given without indication clarity.
- Skipping pre-dose hold-parameter review (vitals/labs/PRN baseline) → avoidable physiologic deterioration risk.
- Delayed documentation and response reassessment → poor continuity and missed deterioration.
- AM/PM versus military-time mismatch during right-time check → early/late or duplicate-dose risk.
- Applying routine timing windows to time-critical medications → subtherapeutic levels and avoidable treatment failure risk.
Related
- medication-administration-documentation-and-reassessment - Covers right documentation and right response in detail.
- oral-medication-administration-safety - Applies route-specific administration checks.
- intravenous-medication-administration-safety - Adds high-alert safeguards for IV delivery.