Obtain a 12-Lead ECG
Key Points
- Pre-procedure checks include order verification, baseline clinical context, and correct demographic entry.
- Accurate lead placement and motion control during capture are essential for diagnostic-quality tracings.
- Abnormal findings require immediate bedside reassessment and prompt provider/emergency escalation.
Equipment
- Provider order for 12-lead ECG
- 12-lead ECG machine with recording paper
- Limb and precordial electrodes
- Skin-prep supplies for oil/moisture/hair removal
Procedure Steps
- Verify the order for 12-lead ECG.
- Collect relevant pretest context: age, sex, cardiac medications, recent blood pressure, and pain level.
- Introduce yourself, perform hand hygiene, verify two identifiers/allergies, explain the procedure, and provide privacy.
- Enter required demographic data into the ECG system.
- Prepare lead sites by removing oil, moisture, and excess hair.
- Open electrodes, confirm they are not expired, and apply four extremity electrodes as labeled.
- Palpate intercostal spaces before placing chest leads; V1 is the only precordial lead placed to the right of the sternum and V1/V2 are commonly placed too high without palpation.
- Place precordial leads:
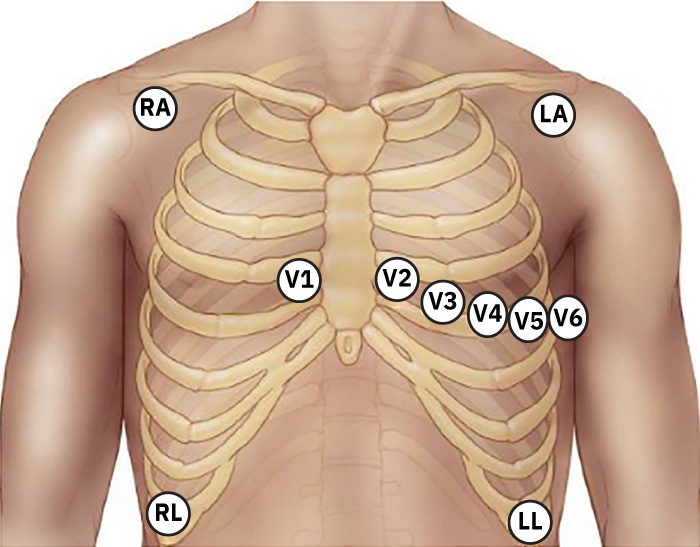 Illustration reference: OpenStax Clinical Nursing Skills Ch.18.3.
Illustration reference: OpenStax Clinical Nursing Skills Ch.18.3.
- V1: fourth intercostal space, right sternal border.
- V2: fourth intercostal space, left sternal border.
- V3: midway between V2 and V4.
- V4: fifth intercostal space, midclavicular line.
- V5: left anterior axillary line, same horizontal level as V4.
- V6: midaxillary line, same horizontal level as V4 and V5.
- Press auto and record ECG while asking the patient to remain still.
- Review printout quality; treat machine interpretation as preliminary and ensure provider review.
- If abnormal pattern is present, assess level of consciousness, carotid pulse, chest pain, and dyspnea; activate emergency support if indicated.
- Remove electrodes, clean skin, reassess for redness/irritation, then perform hand hygiene.
- Restore comfort/safety and notify the provider of abnormalities.
Common Errors
- Incorrect V-lead placement → misleading localization and interpretation errors.
- Misidentifying intercostal spaces (especially placing V1/V2 too high) → systematic precordial interpretation error.
- Recording with patient motion → artifact and poor-quality tracing.
- Relying only on machine interpretation → delayed recognition of clinical instability.
- Failing to reassess unstable symptoms after abnormal ECG → escalation delay in high-risk events.
Related
- ecg-waveform-basics-and-12-lead-application - Conceptual basis for waveform interpretation after acquisition.
- systematic-ecg-interpretation-and-dysrhythmia-triage - Structured rhythm and instability triage after tracing capture.