Measuring Blood Pressure (Manual and Automatic Methods)
Key Points
- Correct cuff size and arm positioning are required for valid blood-pressure readings.
- Blood pressure is documented as systolic/diastolic: systolic during ventricular contraction, diastolic during ventricular filling/rest.
- Manual and automatic methods both require premeasurement rest and proper technique.
- Unexpected values should be rechecked and correlated with symptoms before escalation.
- Severe hypotension can signal shock and inadequate organ perfusion; severe hypertension increases vascular-event risk.
- Mean arterial pressure (MAP) is a perfusion indicator; sustained MAP below about
60 mmHgcan indicate ischemia risk.- When manual/automatic methods are not feasible, Doppler blood pressure (typically systolic only) or invasive arterial-line monitoring may be required in critical care contexts.
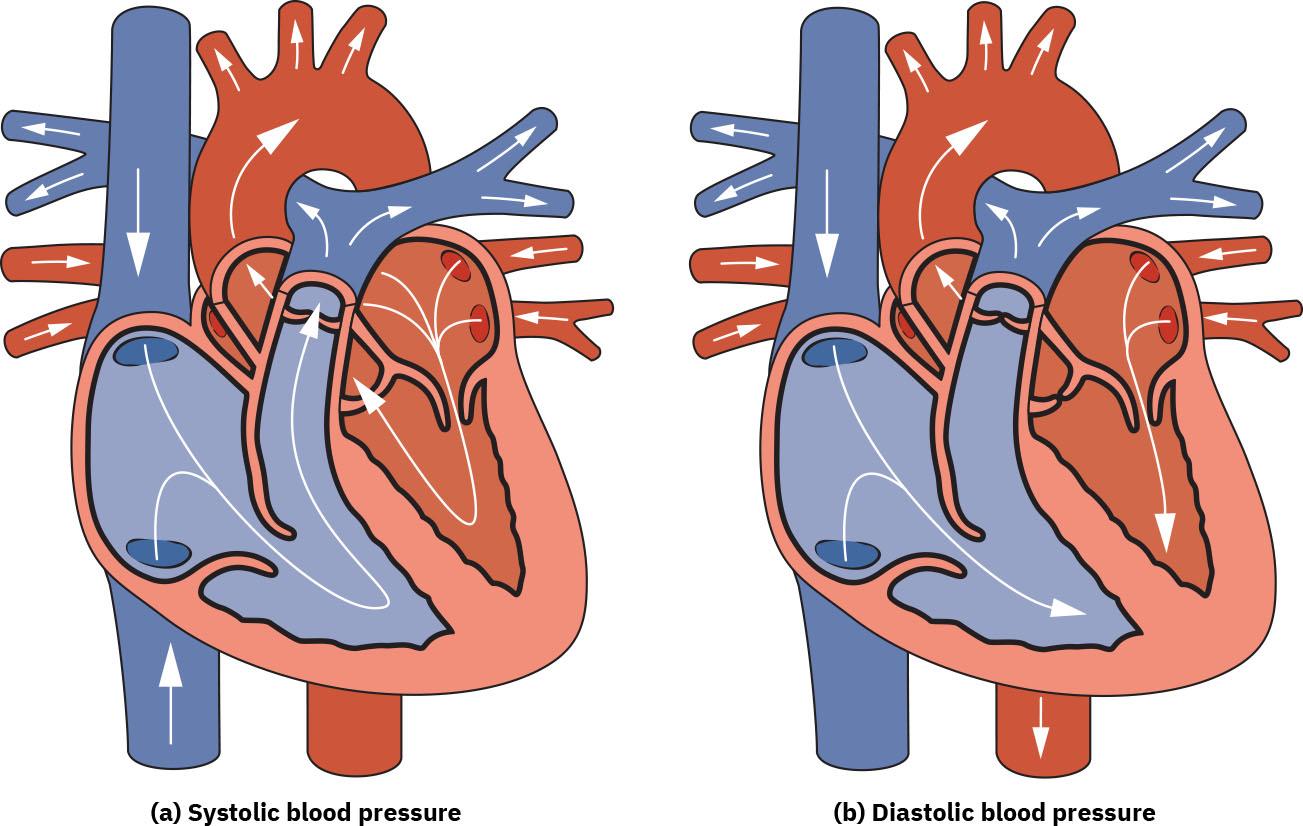 Illustration reference: OpenStax Fundamentals of Nursing Ch.7.1.
Illustration reference: OpenStax Fundamentals of Nursing Ch.7.1.
Equipment
- Appropriately sized blood-pressure cuff
- Manual sphygmomanometer and stethoscope (for manual method)
- Automatic blood-pressure monitor (for automatic method)
- Hand hygiene supplies
Procedure Steps
- Complete routine pre-procedure actions: knock, identify resident, explain procedure, provide privacy, and perform hand hygiene.
- Clean/disinfect the stethoscope and blood-pressure cuff before skin contact per facility policy.
- Before cuff placement, complete focused subjective blood-pressure screening: prior hypertension diagnosis/treatment, current BP medications (including herbs/supplements), usual BP range, and home-monitoring method/timing/site when used.
- Ask about current high/low BP-related symptoms (for example severe headache, dizziness with position change, light-headedness, or fainting episodes) and escalate urgent cues per policy.
- Confirm no contraindicated arm and inspect for local restrictions (for example fistula, current IV line, lymphedema, active/past clot concern, wound, post-mastectomy/lymph-node dissection, stroke-related weakness/restriction, implanted birth-control arm site, or provider restriction).
- If both arms are clinically acceptable, ask patient preference for measurement arm; if restrictions exist, measure blood pressure on an appropriate alternative extremity per policy/provider guidance.
- Seat or position patient with back supported, feet flat, legs uncrossed, and arm supported at heart level; avoid conversation during measurement and allow at least 5 minutes of quiet rest (avoid caffeine/smoking for about 30 minutes when feasible).
- Select cuff size so cuff coverage is about 80 percent of upper-arm length and internal bladder width is about 40 percent of arm circumference; confirm cuff range/index markings fall within the indicated margin on the arm.
- Expose upper arm and apply cuff directly on skin with artery marker centered over brachial artery and lower cuff margin about 1 in (2.5 cm) above the antecubital fossa (adult cuff commonly regular or large based on arm size).
- Manual method: palpate/auscultate brachial artery, inflate cuff to at least about 30 mmHg above the point where the radial pulse disappears, rapidly deflate after palpatory estimate, wait about 30 seconds, then reinflate and deflate slowly (no faster than about 2-3 mmHg/second) while identifying first Korotkoff sound (systolic) and last Korotkoff sound (diastolic).
- Automatic method: start device and keep patient still and silent until reading completes (cuff inflates then deflates automatically before digital display appears); avoid relying on automatic readings when rapid/irregular rhythm (for example atrial fibrillation) or tremor is present.
- If reading is unexpectedly high/low, repeat measurement after brief rest and confirm with manual cuff measurement when feasible; if an automated reading is elevated, follow up with a manual reading.
- Restore patient comfort and environment safety (bed low/locked and call light in reach as applicable).
- Clean/disinfect the stethoscope and blood-pressure cuff after use per policy, then perform hand hygiene.
- Document value, method, cuff size/site, patient position (sitting/standing/lying), and follow-up action.
- For expected findings, document concise baseline details (for example
120/80, left arm, seated, manual cuff). For unexpected findings, document both initial and repeat readings (including side/site and rest interval), associated symptom assessment, relevant hypertension history/medication context, provider notification, and new orders received.
Special Methods
Doppler blood pressure: Use when peripheral pulses are difficult to palpate or special circulatory conditions limit standard methods; cuff inflation/deflation is performed as usual, and the pressure at return of Doppler pulse sound is recorded as systolic pressure.Older-adult auscultation support: In clinically stable older adults with difficult Korotkoff auscultation, Doppler-assisted systolic measurement can improve capture reliability per policy.Arterial-line monitoring: Invasive continuous monitoring used in selected critically ill patients for real-time pressure trending and frequent arterial sampling, managed with advanced critical-care protocols (for example transducer leveling/zeroing and waveform quality checks).
Interpretation Notes
- Common adult category reference:
Normal: systolic 90-119 and diastolic 60-80.Elevated: systolic 120-129 and diastolic 80 or lower.Stage 1 hypertension: systolic 130-139 or diastolic 80-89.Stage 2 hypertension: systolic 140-179 or diastolic 90-119.Hypertensive crisis: systolic 180 or higher or diastolic 120 or higher.
- Diagnostic-label caution: formal hypertension diagnosis is generally based on averaged readings from two or more measurements across two or more occasions per provider guideline use.
- Pulse pressure (
systolic - diastolic) is commonly about40 mmHg; marked narrowing or widening can indicate hemodynamic or vascular pathology and should be trended with the full clinical picture. - Mean arterial pressure can be approximated as
diastolic + 1/3 (systolic - diastolic)and helps estimate average arterial perfusion pressure. - Blood pressure reflects three linked determinants: cardiac contractile force, vascular diameter/tone, and circulating blood volume.
- Emotional distress, dietary stimulant load (for example sodium, caffeine, alcohol), and chronic disease burden (for example kidney or autoimmune vascular effects) can shift readings and should be interpreted in context.
- Transient elevation can occur with recent exertion, anxiety, or white-coat response; repeat after rest before final interpretation.
- Severe vasodilation states (for example septic/anaphylactic patterns) can cause profound hypotension, while hypovolemia lowers pressure through reduced circulating volume.
- Confirm unexpected values with repeat measurement and symptom correlation before concluding true instability.
- Life-span note: routine blood-pressure measurement is generally not performed under age 3 unless cardiac-risk concerns or provider indication is present.
Common Errors
- Using cuff that is too small → falsely high blood pressure.
- Unsupported arm or crossed legs → inaccurate elevation of readings.
- Measuring immediately after activity or conversation → unreliable baseline value.
- Stopping at an auscultatory gap → falsely low systolic or inaccurate diastolic interpretation.
- Failing to recheck abnormal reading → delayed recognition of true instability.
- Relying only on automatic readings in irregular rhythm/tremor contexts → higher risk of inaccurate values and delayed correction.
Related
- measuring-radial-pulse - Pulse and blood pressure trends should be interpreted together.
- vital-sign-indicators-of-physiologic-functioning-and-homeostasis - Links blood-pressure changes to integrated homeostasis assessment.