Measuring Radial Pulse
Key Points
- Radial pulse is counted at the wrist using fingertip palpation for a full 60 seconds.
- A complete 60-second count improves accuracy, especially when rhythm is irregular.
- In adults, radial pulse is the routine preferred site; if inaccessible, apical auscultation is used to validate rate.
- Pulse assessment should include rate, rhythm, force (0 to 3+ scale), and side-to-side equality when relevant.
- Carotid assessment is reserved for urgent checks and is palpated one side at a time.
- In emergencies with suspected poor perfusion, assess central pulses (for example carotid or femoral) before relying on weak peripheral sites.
- Prompt documentation and nurse notification of abnormal findings are required.
Equipment
- Watch or clock with second hand
- Hand hygiene supplies
Site Selection Notes
Radial: Preferred site for routine adult pulse assessment.Apical: Use when radial pulse is inaccessible or when peripheral findings are weak/too rapid/irregular; auscultate for 60 seconds (for example before digoxin administration).Carotid: Used in emergency pulse checks; palpate only one side at a time.Brachial: Preferred upper-extremity peripheral pulse site in infants.Pediatric note: Radial palpation is often less reliable in children under about 5 years; brachial or apical assessment is commonly preferred.Dorsalis pedis: Common lower-extremity peripheral site in adults and children.
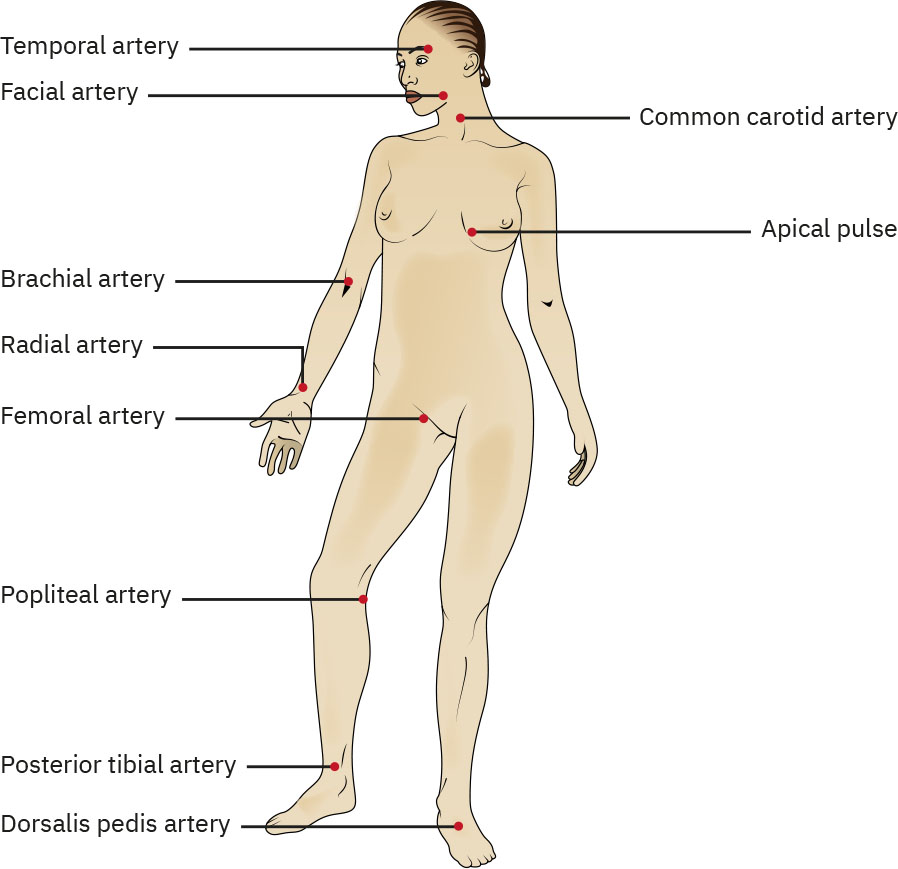 Illustration reference: OpenStax Fundamentals of Nursing Ch.7.2.
Illustration reference: OpenStax Fundamentals of Nursing Ch.7.2.
Procedure Steps
- Perform routine pre-procedure actions: knock, identify resident, explain procedure, provide privacy, and perform hand hygiene.
- Position resident seated comfortably with arms and legs uncrossed when possible; support forearm with palm up.
- Place index and middle fingertips (not thumb) on radial artery at thumb side of wrist, just inside the radial bone.
- Palpate pulse quality (rhythm and volume/force) and begin timing.
- Count beats for 60 seconds.
- Compare right and left radial pulse force when indicated to assess pulse equality.
- If pulse is difficult to detect, consider Doppler-assisted assessment and escalate persistent absent/weak findings with perfusion cues (for example coolness, mottling, severe pain).
- Ensure resident comfort after measurement and restore environment safety (bed low/locked and call light in reach as applicable).
- Perform hand hygiene.
- Document pulse rate, rhythm, force, and resident position (especially if obtained while lying down), and report abnormal findings to nurse.
Common Errors
- Using thumb to palpate pulse → may count examiner’s own pulse.
- Counting for less than 60 seconds in irregular rhythm → inaccurate rate estimate.
- Excessive pressure over artery → can dampen pulse and cause false low count.
- Delayed reporting of abnormal rate/rhythm → delayed clinical intervention.
Related
- measuring-respirations - Pulse and respirations are often assessed together in vital-sign workflow.
- documenting-and-reporting-data - Accurate time-stamped charting supports trend interpretation and escalation.