Airway Adjuncts
Key Points
- Airway adjuncts maintain upper airway patency and are commonly used when mask ventilation is difficult.
- Major adjuncts in this section are oropharyngeal-airway (OPA), nasopharyngeal-airway (NPA), and laryngeal-mask-airway (LMA).
- Correct sizing and insertion technique determine effectiveness and safety.
- NPA is useful when gag reflex is intact or oral access is limited.
Pathophysiology
Upper airway obstruction often occurs when soft tissues, including the tongue, reduce pharyngeal lumen during depressed consciousness or critical illness. Airway adjuncts create or preserve a passage for airflow until spontaneous airway control improves or definitive airway management is established.
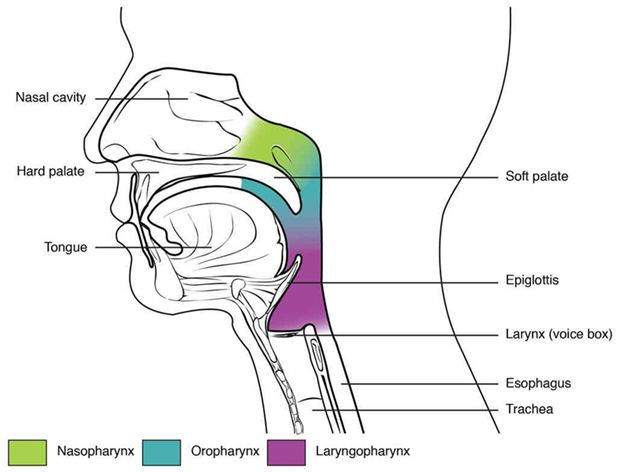 Illustration reference: OpenRN Respiratory Therapy Ch.2.1.
Illustration reference: OpenRN Respiratory Therapy Ch.2.1.
These devices support oxygenation and ventilation by reducing upper-airway resistance and improving manual ventilation mechanics. Inadequate selection or poor placement can worsen obstruction, delay ventilation, and increase tissue trauma risk.
Classification
- OPA: Oral device from lips to pharynx that prevents posterior tongue collapse.
- NPA: Nasal passage airway with a flared end; tolerated in patients with intact gag reflex, trismus, or oral trauma.
- LMA: Supraglottic device positioned above the vocal cords as a more secure airway alternative in selected settings.
Nursing Assessment
NCLEX Focus
Questions often ask which adjunct is most appropriate based on gag reflex, access limitations, and urgency of airway support.
- Assess airway patency and difficulty of mask ventilation before and after adjunct insertion.
- Identify patient factors that guide selection, including oral trauma, trismus, and gag reflex status.
- Verify sizing landmarks before insertion to reduce malposition risk.
- Reassess ventilation effectiveness and oxygenation trends immediately after placement.
Nursing Interventions
- Select device type and size using source-described landmarks before insertion.
- Use gentle technique and correct orientation during OPA/NPA placement.
- Apply water-soluble lubrication for NPA insertion to reduce nasal trauma.
- Confirm position and monitor for persistent obstruction or inadequate ventilation.
- Escalate to advanced-airways-and-intubation if adjunct-supported ventilation remains inadequate.
Placement Safety
Incorrect sizing or forceful insertion can cause ineffective ventilation, mucosal injury, and delayed airway stabilization.
Pharmacology
No specific medication regimen is defined in this source section; the focus is device-based airway support and placement technique.
Clinical Judgment Application
Clinical Scenario
A patient with deteriorating ventilation has difficult mask ventilation and cannot maintain upper airway patency.
- Recognize Cues: Poor mask seal effectiveness, obstructed airflow, and continued respiratory compromise.
- Analyze Cues: Upper airway collapse is likely limiting effective ventilation.
- Prioritize Hypotheses: Immediate need is airway adjunct placement matched to patient tolerance and anatomy.
- Generate Solutions: Choose OPA, NPA, or LMA based on exam findings and insertion feasibility.
- Take Action: Insert selected adjunct with correct sizing and technique, then reassess ventilation.
- Evaluate Outcomes: Airflow, chest rise, and oxygenation improve or escalation pathway is activated.
Related Concepts
- airway-adjunct-insertion - Procedure-level steps for sizing and placement.
- bag-valve-mask-manual-ventilation - Adjuncts improve mask ventilation performance.
- manual-resuscitators-and-manual-ventilation - Manual ventilation context for adjunct use.
- respiratory-failure - Frequent clinical indication for adjunct-supported ventilation.
- advanced-airways-and-intubation - Escalation when adjuncts do not provide adequate airway control.
Self-Check
- Which findings support choosing NPA over OPA in an unstable patient?
- Why is pre-insertion sizing a priority step for both OPA and NPA?
- When should care escalate from basic airway adjuncts to advanced airway intervention?