Bag Valve Mask Manual Ventilation
Key Points
- Use BVM for respiratory arrest or inadequate breathing, and select the correct bag-mask size to reduce lung injury.
- Set oxygen flow to 15 L/min when connected to oxygen, which delivers approximately 100% FiO2.
- Deliver breaths only until visible chest rise, with each breath over about 1 second, to reduce gastric inflation and lung trauma.
- Two-rescuer technique is preferred when possible because one rescuer can maintain a leak-proof mask seal and jaw thrust while the other controls bag timing and depth.
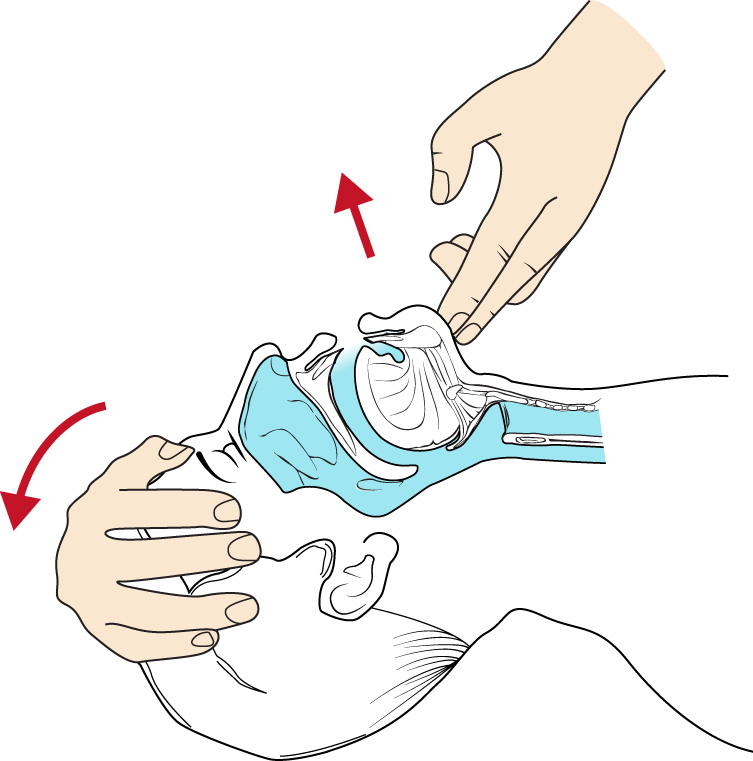 Illustration reference: OpenStax Medical-Surgical Nursing Ch.33.1.
Illustration reference: OpenStax Medical-Surgical Nursing Ch.33.1.
Equipment
- Appropriately sized bag valve mask (adult, child, or infant)
- Oxygen source with flowmeter set to 15 L/min
- Optional exhaust-port filter to reduce spread of airborne infection
Procedure Steps
- Identify absent or inadequate breathing and position the patient supine on a firm surface.
- Select the appropriate mask and bag size for the patient.
- Connect the BVM to oxygen and set flow to 15 L/min; add an exhaust filter if available.
- Position at the head of the patient with shoulders square to the patient.
- Place the mask using the non-dominant hand, with the nose portion over the bridge of the nose and mask over the mouth.
- Create the mask seal using the E/C technique: keep thumb and index finger on the hard mask shell (C), with remaining fingers lifting the jaw (E).
- Maintain head tilt in a sniffing position while preserving a leak-proof seal.
- Squeeze the bag with the dominant hand until chest rise is visible.
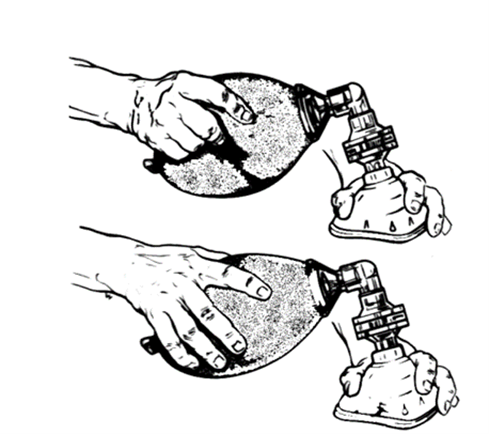 Illustration reference: OpenRN Respiratory Therapy Ch.1.1.
Illustration reference: OpenRN Respiratory Therapy Ch.1.1.
- Deliver each breath over 1 second, then ventilate at ordered emergency cadence (adult about every 5-6 seconds; pediatric guidance in this source ranges from every 3 seconds to every 2-3 seconds).
- Prefer a two-rescuer approach when possible: one rescuer maintains seal and jaw thrust, and the other controls bag timing and depth.
- When one rescuer is sealing the mask, lock elbow and lean back slightly to bring the patient’s face into the mask while preserving jaw lift.
- Coordinate breaths with patient inhalation if the patient is still breathing to avoid asynchrony.
- Continue until airway and ventilation stabilize or advanced airway management is established.
Common Errors
- Poor mask seal → inadequate tidal volume and poor oxygenation.
- Excessive squeeze volume or pressure → gastric inflation, aspiration risk, and lung injury.
- Incorrect breath timing → breath stacking or patient-ventilator asynchrony.
- One-rescuer fatigue during prolonged use → reduced ventilation quality over time.
- Gripping soft mask edges instead of hard shell during E/C technique → unstable seal and air leak.
Related
- airway-adjuncts - Adjunct devices can improve airway patency during manual ventilation.
- advanced-airways-and-intubation - Endotracheal intubation may replace mask ventilation when prolonged support is needed.