Prenatal Development Phases and Teratogen Vulnerability Windows
Key Points
- Prenatal development progresses through germinal, embryonic, and fetal phases with distinct risks.
- Organogenesis in the embryonic phase carries the highest teratogen-related structural-risk window.
- Fetal phase emphasizes maturation of already formed systems and preparation for extrauterine life.
- Nurses reduce risk through early education, exposure review, and timely prenatal follow-up.
Pathophysiology
After conception, zygote division and implantation establish early viability. During the pre-embryonic (germinal) period, the fertilized ovum progresses from zygote to morula (about 16-cell stage), then blastocyst and trophoblast before implantation.
In the embryonic phase (approximately week 2 through week 8 postconception), cell-layer differentiation (ectoderm, mesoderm, endoderm) drives organ-system formation, making this period highly vulnerable to disruptive exposures. Because one layer contributes to multiple structures, a single-layer developmental disruption can produce multi-organ effects (for example renal and ear anomalies from mesoderm-related disruption).
During the fetal period (about week 9 to birth), systems continue growth and functional maturation (for example pulmonary and neurologic readiness), while ongoing maternal conditions and exposures still influence outcomes. Common stage anchors include detectable sex characteristics by around 16 weeks, breathing movements by around 24 weeks, surfactant development near 28 weeks, and sucking-reflex emergence near 32 weeks, with full term around 40 weeks.
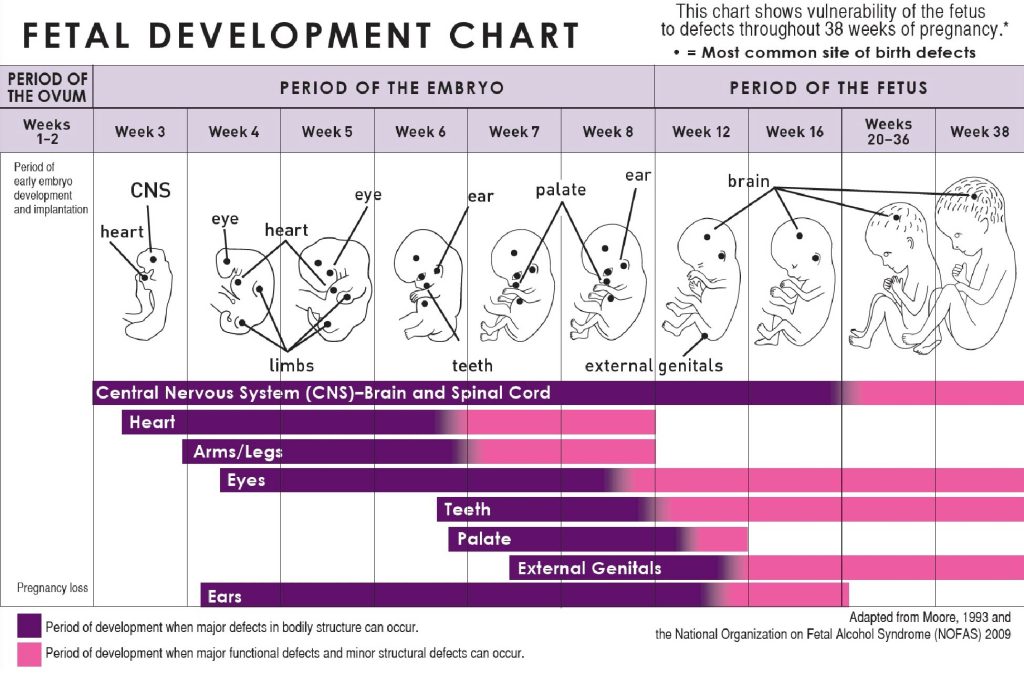 Illustration reference: OpenRN Nursing Health Promotion Ch.8.4.
Illustration reference: OpenRN Nursing Health Promotion Ch.8.4.
Because organogenesis is sequence-specific, exposure during narrow windows can produce targeted structural defects (for example foregut separation errors such as tracheoesophageal fistula).
Classification
- Pre-embryonic/germinal phase: Conception to implantation and early cellular replication.
- Embryonic phase: Organogenesis-focused development with highest structural-defect susceptibility.
- Fetal phase: Growth and function maturation until birth.
- Early structural sequence: Zygote → morula → blastocyst/trophoblast → implantation.
- Risk domains: Teratogens, maternal infection, chronic disease, nutrition deficiency, and toxic exposure.
Nursing Assessment
NCLEX Focus
Exposure timing is as important as exposure type when estimating fetal risk.
- Assess gestational age accurately before interpreting risk, recognizing that clinical gestational weeks are conventionally counted from the first day of the last menstrual period.
- Assess medication, substance, infection, and environmental exposure history.
- Assess maternal chronic-condition control and nutrition status.
- Assess warning signs requiring urgent prenatal escalation.
Nursing Interventions
- Provide stage-specific education on avoidable teratogen exposure.
- Coordinate prenatal screening and follow-up based on risk profile.
- Reinforce nutrition and supplementation guidance aligned to gestation stage.
- Support shared decision-making with clear risk-benefit explanation.
Exposure-Timing Misinterpretation
Underestimating early gestational exposure risk can delay critical evaluation and counseling.
Pharmacology
Medication safety during pregnancy requires trimester-aware risk review and the lowest effective exposure strategy consistent with maternal health needs.
Clinical Judgment Application
Clinical Scenario
A newly pregnant patient reports unplanned first-trimester exposure to a potentially teratogenic medication.
- Recognize Cues: Time-sensitive exposure during high-vulnerability period.
- Analyze Cues: Embryonic-stage risk may require targeted evaluation and counseling.
- Prioritize Hypotheses: Immediate need is accurate risk stratification and maternal safety planning.
- Generate Solutions: Coordinate specialist consultation and exposure-informed surveillance.
- Take Action: Update medication plan and provide structured follow-up guidance.
- Evaluate Outcomes: Improved maternal-fetal safety with informed decision-making.
Related Concepts
- growth-vs-development-lifespan-milestones-and-play-patterns - Lifespan context beginning with prenatal phase.
- well-care-anticipatory-guidance-and-immunization-across-the-lifespan - Preventive framework spanning prenatal to adolescence.
- fetal-growth-and-development - Detailed fetal stage physiology and monitoring.
- preconception-teratogen-and-medication-exposure-review - Upstream risk-reduction before conception.
- preexisting-conditions-placing-delivery-at-risk - Maternal-fetal risk integration.
Self-Check
- Why is embryonic development the highest-risk window for structural teratogenic effects?
- How does gestational-age accuracy change nursing risk interpretation?
- Which exposures require immediate prenatal escalation?