Tracheoesophageal Fistula
Key Points
- TEF involves an abnormal fistula tract connecting the esophagus and trachea; esophageal atresia (EA) is the incomplete formation of the esophagus.
- The hallmark clinical presentation is the “three C’s”: coughing, choking, and cyanosis during feeding.
- Diagnosis is confirmed by inability to pass an orogastric catheter and chest/abdominal x-ray.
- Surgical correction is required; preoperatively, the neonate is NPO with parenteral nutrition.
Pathophysiology
TEF results from a developmental error in lateral septation of the foregut that forms the esophagus and trachea. The fistula tract connecting these structures is thought to arise from a defective branch of the embryonic lung due to abnormal epithelial-mesenchymal interactions. The connection allows air to enter the stomach and oral liquids to cross into the trachea, causing aspiration. Several anatomical variants exist, with the most common being a proximal esophageal atresia with a distal tracheoesophageal fistula (Gross type C, approximately 85% of cases).
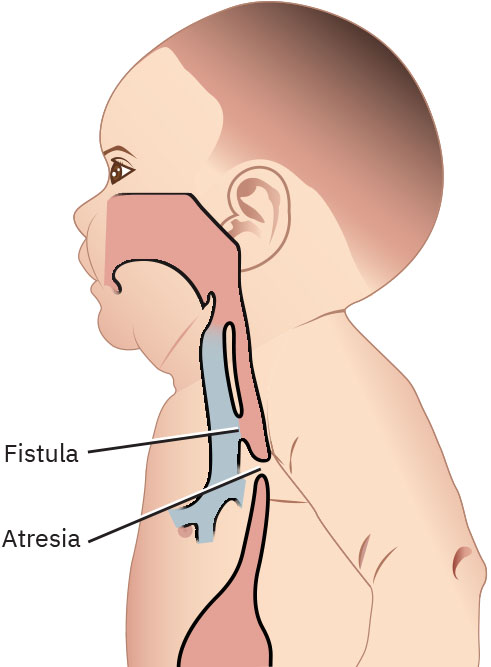 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.25.2.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.25.2.
Clinical Manifestations
- Excessive drooling and oral secretions.
- The “three C’s” during feeding: coughing, choking, and cyanosis.
- Abdominal distension (air passes through the fistula into the stomach).
- Inability to swallow saliva or feedings.
- Recurrent aspiration pneumonia.
Nursing Assessment
- Assess for the three C’s during first feeding attempt.
- Attempt to pass an orogastric or nasogastric catheter; inability to advance confirms esophageal atresia.
- Review x-ray findings: coiled catheter in the proximal esophageal pouch, gas-filled stomach (distal TEF).
- Monitor respiratory status: oxygen saturation, breath sounds, signs of aspiration.
- Assess associated anomalies (VACTERL association: vertebral, anorectal, cardiac, tracheoesophageal, renal, limb defects).
Nursing Interventions
- Maintain NPO status preoperatively; suction proximal esophageal pouch to prevent aspiration.
- Position the neonate with the head of the bed elevated to reduce gastric reflux through the fistula.
- Provide parenteral nutrition (PPN or TPN) until surgical correction and feeding can begin.
- Postoperative care: ventilatory support and weaning, monitor esophagram results (approximately postoperative day 5) for surgical leak.
- Begin oral feeds only after radiographic confirmation of intact surgical repair.
- Administer prescribed antireflux medications postoperatively.
- Educate parents about the surgical plan, expected NICU course, and long-term feeding considerations.
Related Concepts
- congenital-heart-defects-acyanotic-and-cyanotic-patterns - Cardiac anomalies in VACTERL association.
- aspiration-pneumonia - Complication from esophageal-tracheal communication.
- neonatal-bonding-feeding-and-newborn-screening - Early identification of congenital anomalies.
- gastroschisis - Another congenital GI anomaly requiring neonatal surgery.
- parenteral-nutrition-monitoring - Nutritional support during NPO period.
Self-Check
- What are the “three C’s” that characterize TEF/EA presentation during feeding?
- How is esophageal atresia confirmed diagnostically?
- Why should the neonate with TEF be positioned with the head of the bed elevated?