Maternal Substance Use During Pregnancy
Key Points
- Substance use disorder in pregnancy is a high-risk condition linked to maternal and fetal morbidity and mortality.
- Universal prenatal screening with validated tools is recommended because self-disclosure barriers are common.
- SURP positive screens (moderate/high risk) require follow-up assessment and intervention.
- SBIRT provides a structured pathway: screening, brief motivational intervention, and referral to treatment.
- Drug/alcohol testing has legal and economic implications; informed consent, confirmatory testing, and state-law awareness are essential.
- Pregnancy counseling should explicitly include nicotine/vaping, alcohol, marijuana, opioids, and other illicit drugs because each carries distinct maternal-fetal risks.
- Cocaine and methamphetamine use increase risk of migraine, seizure, prelabor rupture of membranes, and placental abruption.
Pathophysiology
Substance use disorder is a clinically significant pattern of alcohol or drug use that activates reward pathways and impairs judgment, self-care, and role function. During pregnancy, ongoing exposure increases risk for obstetric and neonatal complications, including fetal alcohol spectrum disorder and neonatal abstinence syndrome.
Behavioral and structural barriers (stigma, fear of legal consequences, limited treatment awareness, and low trust in care systems) can delay disclosure and treatment entry.
Classification
- Low-risk screen: No affirmative SURP risk responses.
- Moderate-risk screen: One affirmative SURP item; requires further assessment.
- High-risk screen: Two or three affirmative SURP items; requires urgent follow-up and treatment linkage.
- Co-occurring risk context: Concurrent mental-health disorders and IPV requiring integrated prenatal care planning.
Nursing Assessment
NCLEX Focus
Use private, nonjudgmental, universal screening; do not rely only on spontaneous disclosure.
- Screen all pregnant clients with validated tools per protocol (for example 4 P’s or SURP).
- When available, use validated tool options matched to setting/workflow (for example 4P’s, NIDA Quick Screen, CRAFFT, and SURP-context instruments).
- Screen specific exposure categories: tobacco/vaping nicotine, alcohol, marijuana, opioids, and other illicit substances, including timing since pregnancy recognition.
- Use SURP question domains: marijuana history, alcohol use before pregnancy recognition, and perceived need to cut down.
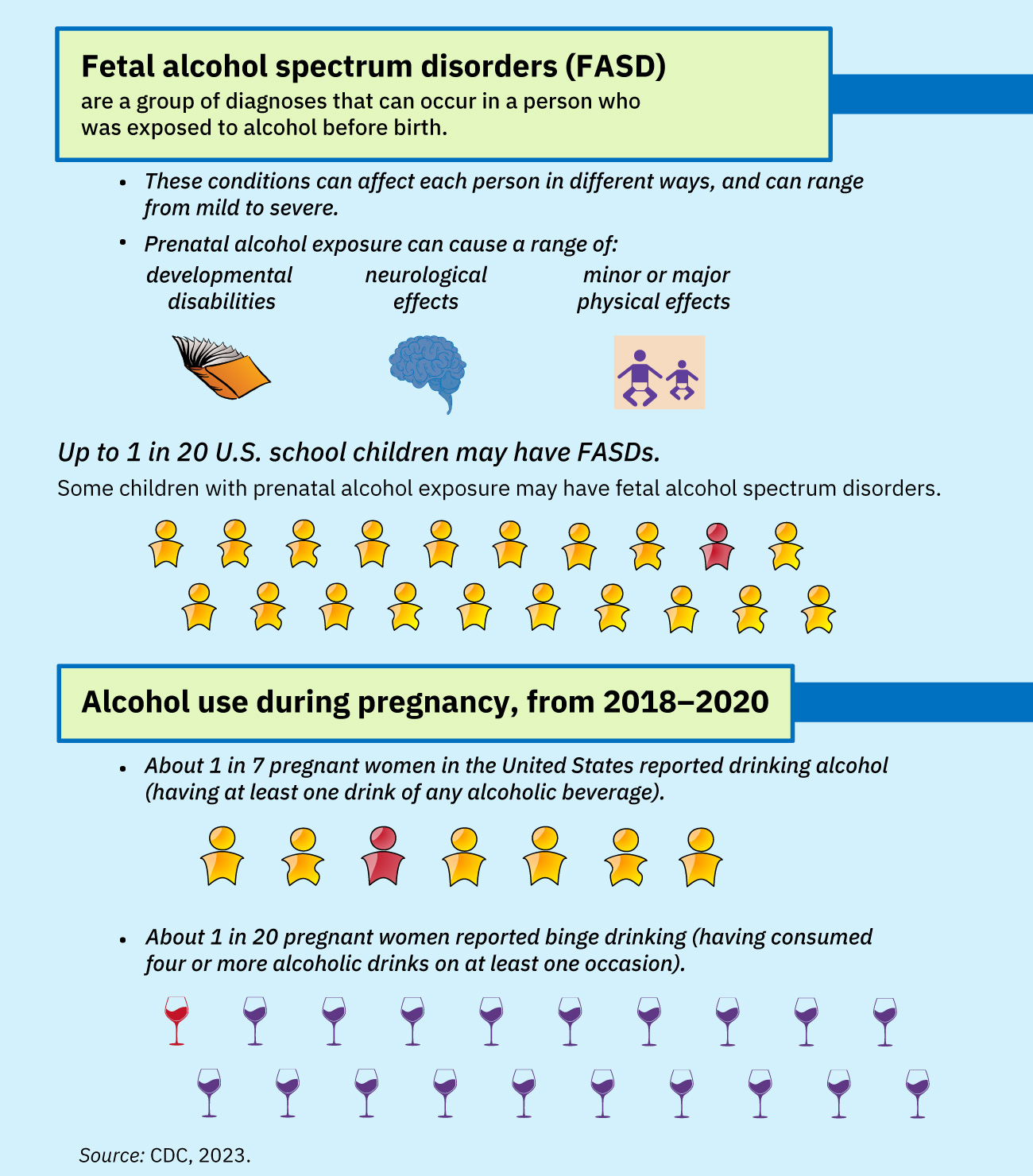 Illustration reference: OpenStax Clinical Nursing Skills Ch.20.2.
Illustration reference: OpenStax Clinical Nursing Skills Ch.20.2.
- Classify screen results and document objective risk level for follow-up planning.
- Assess barriers to disclosure and treatment engagement (stigma, legal concerns, hopelessness, limited knowledge).
- Assess additional gendered barriers (for example child-custody fear, caregiving-role pressure, and limited access to women-focused treatment programs).
- Assess co-occurring depression, anxiety, trauma, and IPV because these commonly overlap with prenatal substance misuse.
- If laboratory testing is considered, verify informed-consent requirements and state-specific testing/reporting rules.
- Confirm that positive initial toxicology screens are followed by confirmatory testing to reduce false-positive harm.
- During labor, assess for possible acute intoxication and associated obstetric instability.
Nursing Interventions
- Implement SBIRT after positive screening to improve insight and readiness for behavior change.
- Deliver brief intervention with non-stigmatizing communication and motivational interviewing principles.
- Notify the provider of positive screens and coordinate referral to counseling, recovery services, and community resources.
- Provide patient education on maternal-fetal risks and harm-reduction steps while treatment is being initiated (for example low birth weight, preterm birth, placental abruption, fetal demise, neonatal withdrawal, SIDS, and neurodevelopmental effects).
- In opioid-use disorder, support medication-for-opioid-use-disorder referral (for example methadone or buprenorphine pathways) to reduce relapse and unmanaged withdrawal risk.
- Reinforce postpartum newborn monitoring needs when prenatal opioid or sedative exposure is present because withdrawal may emerge after birth.
- Coordinate integrated care for co-occurring conditions (mental-health disorders, IPV, social instability).
- Teach that stimulant use should stop immediately in pregnancy and that ongoing stimulant use is a contraindication to breastfeeding.
- If toxicology is obtained per policy and returns positive at delivery, notify newborn care teams (nursery/NICU) for enhanced monitoring planning.
- Document screening results, counseling content, consent status, and referral follow-through.
Legal and Reporting Harm Risk
Substance testing without clear consent/legal workflow can create avoidable legal, economic, and care-access harms.
Pharmacology
Medication decisions are individualized to substance type, withdrawal risk, gestational age, and treatment setting. Nursing priorities are screening-identified escalation, safety monitoring, and linkage to treatment rather than unsupervised medication advice.
Clinical Judgment Application
Clinical Scenario
A prenatal patient screens moderate-risk on SURP and reports fear of legal consequences if substance use is documented.
- Recognize Cues: Positive screening result plus major disclosure barrier.
- Analyze Cues: Without trust and structured follow-up, treatment delay is likely and maternal-fetal risk remains high.
- Prioritize Hypotheses: Immediate priority is confidential, nonjudgmental engagement with SBIRT and referral activation.
- Generate Solutions: Provide brief intervention, explain consent/reporting framework, and initiate treatment-resource linkage.
- Take Action: Coordinate provider notification, referral, and documented follow-up plan.
- Evaluate Outcomes: Patient engages in ongoing care and recovery support with reduced prenatal risk exposure.
Related Concepts
- substance-use-disorders - Core SUD neurobiology and treatment framework underlying prenatal risk.
- opioid-use-disorder - Important subtype with pregnancy and neonatal abstinence implications.
- neonatal-effects-of-prenatal-substance-exposure - Newborn withdrawal and FASD-focused postbirth management priorities.
- domestic-and-intimate-partner-violence - IPV often co-occurs with prenatal substance-use risk and should be co-screened.
- psychosocial-aspects-of-pregnancy - Social stress and stigma strongly influence disclosure and treatment engagement.
Self-Check
- Which SURP result patterns require follow-up intervention?
- Why is SBIRT preferred over one-time counseling after a positive prenatal substance screen?
- Why are confirmatory tests and informed consent critical when prenatal toxicology is performed?