Domestic and Intimate Partner Violence
Key Points
- Domestic violence and IPV include physical, sexual, emotional, and financial abuse within close relationships.
- IPV also includes stalking and coercive psychological aggression used to maintain power and control.
- Survivors may present with subtle patterns rather than direct disclosure.
- IPV frequently follows a repeating cycle of tension building, violent incident, and honeymoon/reconciliation period.
- Severe physical IPV exposure is common across genders (approximately 22 percent of women and 14 percent of men lifetime), with substantial injury and homicide burden.
- Universal, private, trauma-informed screening is a core nursing safety intervention.
- Nursing care prioritizes autonomy, safety planning, and resource linkage instead of directive commands.
- Victims can be women or men and across heterosexual or LGBTQ+ relationships.
- IPV is one of the most prevalent adult safety threats, so early nursing recognition and private screening are high-priority actions.
- In pregnancy, IPV is associated with preterm birth, low birth weight, fetal injury, maternal depression/anxiety/PTSD, and maternal-fetal death risk.
Pathophysiology
IPV produces cumulative physical injury and psychologic trauma through repeated coercion, fear conditioning, isolation, and loss of control. Abuse dynamics often follow repeating escalation and reconciliation patterns that can complicate help-seeking.
Reproductive coercion and sexual violence within IPV can increase unintended pregnancy risk, STI exposure, and long-term reproductive harm. Chronic abuse is also associated with anxiety, depression, sleep disturbance, and somatic symptom burden.
Long-term IPV burden can include chronic cardiovascular, digestive, reproductive, musculoskeletal, and neurologic conditions, and may increase smoking, binge drinking, and risky sexual behaviors.
Classification
- Violence forms: Physical, sexual, emotional/psychologic, financial, and coercive-control behaviors.
- Additional IPV forms: Stalking and nonphysical sexual coercion events (for example coercive sexual messaging).
- Relationship context: Current or former intimate partners and household/family violence overlap.
- Cycle-of-violence domain: Tension building, violent incident, and honeymoon/reconciliation phase with recurrent repetition risk.
- Risk pattern domain: Escalating control behaviors, isolation, and repeated unexplained injuries.
- Clinical impact domain: Immediate safety threats plus chronic trauma-related health consequences.
- Theory-guided education domain: Power-and-control tactics versus equality-based healthy-relationship behaviors.
- Adolescent context: Teen dating violence with elevated risk among LGBTQ+ youth and in substance-involved nonconsensual sexual encounters.
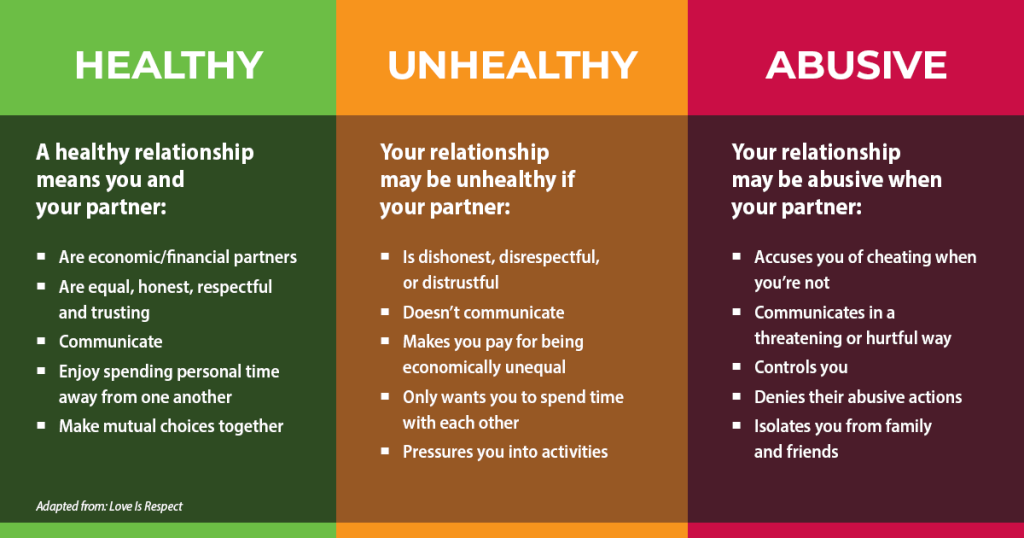 Illustration reference: OpenRN Nursing Health Promotion Ch.6.3.
Illustration reference: OpenRN Nursing Health Promotion Ch.6.3.
Nursing Assessment
NCLEX Focus
Assess privately, normalize screening, and determine immediate danger before any planning discussion.
- Screen all women of childbearing age and other at-risk patients using confidential, direct language.
- Perform routine IPV screening in high-yield entry points, including initial primary-care visits, OB-GYN visits, emergency-department encounters, and hospital admission workflows.
- Assess injuries, delay patterns in care-seeking, recurrent anxiety/depression visits, and partner-controlling behaviors.
- Assess high-suspicion utilization patterns: frequent emergency/urgent-care visits, missed appointments, and delayed treatment despite injury.
- Assess mismatch patterns between reported mechanism and observed injury severity/distribution (for example repeated “falls” with patterned bruising).
- Assess stalking, coercive aggression, and fear-based control dynamics by current or former partners.
- Assess life-course recurrence risk, including prior exposure to family violence in childhood or adolescence.
- Evaluate reproductive coercion, sexual violence, and barriers to leaving.
- Assess pregnancy-relevant warning signs such as late prenatal-care initiation and repeated abortions in coercive-control contexts.
- Assess medication nonadherence related to partner interference with access to prescriptions or medications.
- Determine immediate lethality risk and presence of children/dependents in danger.
- Assess whether the partner is overly attentive, verbally abusive, answers for the patient, or resists leaving the room.
- If privacy cannot be secured safely, avoid forcing disclosure in front of the partner and arrange a safer private re-screening opportunity.
- Use structured pregnancy-compatible screening options when available (for example HITS: four 1-5 items; score above 10 suggests positive IPV screen).
- When using validated IPV risk instruments, confirm the patient is alone and can speak freely before tool administration.
- During focused exam, assess suspicious injury patterns (head/neck/teeth/genital trauma, central-body injuries, defensive forearm wounds, bruises of different ages, possible strangulation signs).
- Assess social isolation, reluctance to undress or undergo genital/rectal/oral exams, and dissociative or flat affect consistent with trauma response.
- Assess near-term repeat-victimization risk because recurrence can occur soon after a prior incident.
- Assess readiness stage and acknowledge that many survivors may not initially choose to leave the relationship.
- Re-screen at later visits when suspicion remains because repeated normalized inquiry can increase disclosure over time.
- Document objective findings and patient statements exactly.
Nursing Interventions
-
Provide validation and avoid blaming or pressuring language.
-
Avoid victim-blaming language (for example “why didn’t you leave”) and frame responsibility on the abusive partner’s behavior.
-
Conduct private, nonjudgmental interview using concise open-ended questions (for example asking about “being hurt” or “treated badly”) and avoid coercive labeling language.
-
Use gentle follow-up questioning and supportive listening when explanations are vague or inconsistent, prioritizing trust-building over immediate disclosure.
-
Assure confidentiality within legal limits, including mandatory-reporting and duty-to-warn exceptions for grave danger.
-
In acute-care settings with high retaliation risk, coordinate confidentiality safeguards (for example controlled room entry/visitor screening and restricted location disclosure) per policy.
-
Do not pressure disclosure, leaving, or filing charges; use shared decision-making and respect survivor pacing.
-
Assist with individualized safety planning (housing, children, work, emergency contacts, documents).
-
Use brief structured screening when appropriate (for example SAFE: Stress/Safety, Afraid/Abused, Friends/Family, Emergency plan).
-
In settings with privacy barriers, consider computer-assisted self-interview workflows to improve confidential disclosure opportunities.
-
Use structured danger-screening support (for example validated danger-assessment tools) when available per policy.
-
Prioritize lethality risk checks: prior strangulation, firearm access, and perpetrator suicidality (threats, prior attempts, specific plan, means access).
-
Consider context-specific validated tools when available (for example ODARA, SHARP, or relationship-violence questionnaires) to strengthen risk stratification.
-
Connect to social work, shelters, counseling, legal resources, and crisis hotlines.
-
Teach abuse-recognition using power-and-control versus equality relationship frameworks when this supports survivor understanding and safety planning.
-
Provide prevention education that reinforces healthy, respectful, nonviolent relationship norms in clinical and community settings.
-
Reinforce CDC-aligned prevention layers when teaching clients and families: healthy-relationship education, bystander/adult engagement, early-home-visitation and parenting supports, protective-environment design, economic supports, and survivor-centered services.
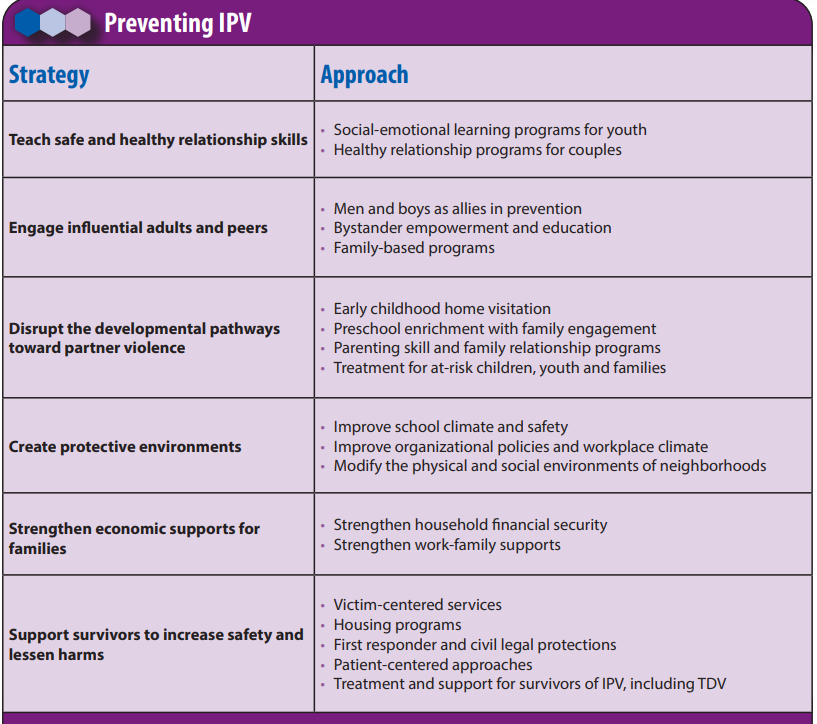 Illustration reference: OpenRN Nursing Health Promotion Ch.6.3.
Illustration reference: OpenRN Nursing Health Promotion Ch.6.3. -
Offer confidential national and local IPV resources (for example domestic violence hotline and trauma-focused referral services).
-
Help clients complete a personalized online safety plan and confirm safe access to hotline resources before discharge.
-
Follow state and institutional reporting requirements.
-
For autonomous competent adults, align reporting with jurisdictional requirements; separately escalate mandated-reporting concerns for children or dependent older adults at risk in the home.
-
In jurisdictions where autonomous competent adult IPV is exempt from routine mandatory reporting, prioritize survivor consent and collaborative safety planning before external reporting unless a separately mandated injury/crime trigger is present.
-
Treat separation as a high-risk period: violence can escalate sharply during and after leaving, with major homicide concentration around separation; complete a personalized safety plan before discharge.
-
Arrange follow-up that protects confidentiality and ongoing safety.
-
Chart injuries with objective descriptors and direct quoted statements; avoid legal conclusions or diagnostic labels in narrative wording.
-
Record exam timestamp and estimated incident-to-exam interval when known to support longitudinal pattern review.
Leave-Now Directive Harm
Telling a survivor to leave immediately without a practical safety plan can increase short-term danger.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| anxiolytics | Acute crisis symptom contexts | Short-term support only; must be paired with safety and psychosocial intervention. |
| antidepressants | Persistent trauma-related mood symptoms | Useful when integrated with counseling and violence-recovery services. |
Clinical Judgment Application
Clinical Scenario
A patient arrives with recurrent bruising, requests rapid discharge, and is accompanied by a partner who refuses to leave the exam room.
- Recognize Cues: Injury pattern and partner control suggest possible IPV.
- Analyze Cues: Disclosure may be unsafe in partner presence.
- Prioritize Hypotheses: Priority is private screening and immediate safety assessment.
- Generate Solutions: Separate patient safely, screen, document, and activate social-work support.
- Take Action: Begin survivor-led safety planning and referral.
- Evaluate Outcomes: Patient receives confidential support and an actionable safety pathway.
Related Concepts
- violence-against-women-incidence-history-and-psychosocial-factors - Epidemiologic and theory foundation for IPV assessment.
- sexual-abuse-and-assault-care - Sexual violence may coexist with IPV.
- psychological-trauma-of-violence-against-women - Mental-health sequelae require longitudinal care.
- therapeutic-communication - Trust and validation improve disclosure.
- culturally-competent-care - Identity-sensitive care reduces barriers to support.
Self-Check
- Which interaction cues suggest coercive control even without direct disclosure?
- Why must safety planning be survivor-led rather than provider-directed?
- What documentation practices best support both care and legal integrity?