Malignant Reproductive Neoplasms
Key Points
- Early detection and prevention are central to improved outcomes in gynecologic cancer care.
- Major cancers in this domain include cervical, ovarian, uterine/endometrial, vulvar, and vaginal malignancies.
- Risk, symptom pattern, and diagnostic approach differ by cancer site, but delayed recognition worsens prognosis.
- Nursing roles span screening education, diagnostic/procedural support, symptom surveillance, and psychosocial care.
Pathophysiology
Malignant neoplasms in reproductive tissues develop through progressive cellular dysplasia and invasive transformation with potential metastasis. Cervical malignancy is strongly linked to oncogenic HPV strains, supporting the preventive role of vaccination and guideline-based screening. Endometrial and uterine malignancies are influenced by prolonged unopposed estrogen exposure patterns.
Ovarian cancer often presents with nonspecific symptoms and is frequently diagnosed at later stages. Vulvar and vaginal cancers are less common but require prompt evaluation of persistent lesions, burning, bleeding, or nonhealing sores.
Clinical screening follow-up uses cervical precancer continuum language (for example LSIL, HSIL, adenocarcinoma in situ) and colposcopy/biopsy pathways when cytology is abnormal. Postmenopausal bleeding remains a major warning sign for endometrial pathology requiring prompt transvaginal imaging and endometrial sampling. For ovarian-risk counseling, protective associations are often discussed for prior anovulation-focused contraceptive use, breastfeeding history, and multiparity, while persistent symptom clusters still require urgent evaluation.
Management depends on site and stage and may include surgery, radiation, chemotherapy, or multimodal treatment. Nursing surveillance for treatment complications and emotional burden is essential throughout the care continuum.
Classification
- Cervical malignancies: HPV-associated dysplasia-to-cancer continuum.
- Uterine/endometrial malignancies: Hormone-linked endometrial pathology and uterine sarcoma variants.
- Ovarian malignancies: Often advanced-stage presentations with broad peritoneal involvement potential.
- Ovarian-stage framework: Stage I confined to ovary/ovaries, Stage II pelvic extension, Stage III nodal or abdominal-lining spread, Stage IV distant metastasis (for example liver or lung).
- Ovarian-screening limitation domain: No routine mortality-reducing screening test is recommended for average-risk populations; evaluate persistent unexplained symptom clusters and high-risk genetic/family history.
- Vulvar/vaginal malignancies: Rare cancers with lesion-focused diagnostic pathways.
- Endometrial-screening domain: Routine asymptomatic screening is not recommended; postmenopausal or unexplained abnormal bleeding requires prompt endometrial evaluation.
- Pregnancy-associated cancer-care domain: Management may require balancing fetal maturity, maternal staging urgency, and ethically complex treatment-timing decisions.
- Breast malignancies: Ductal/lobular pathways with lymphatic and hematogenous metastatic spread potential.
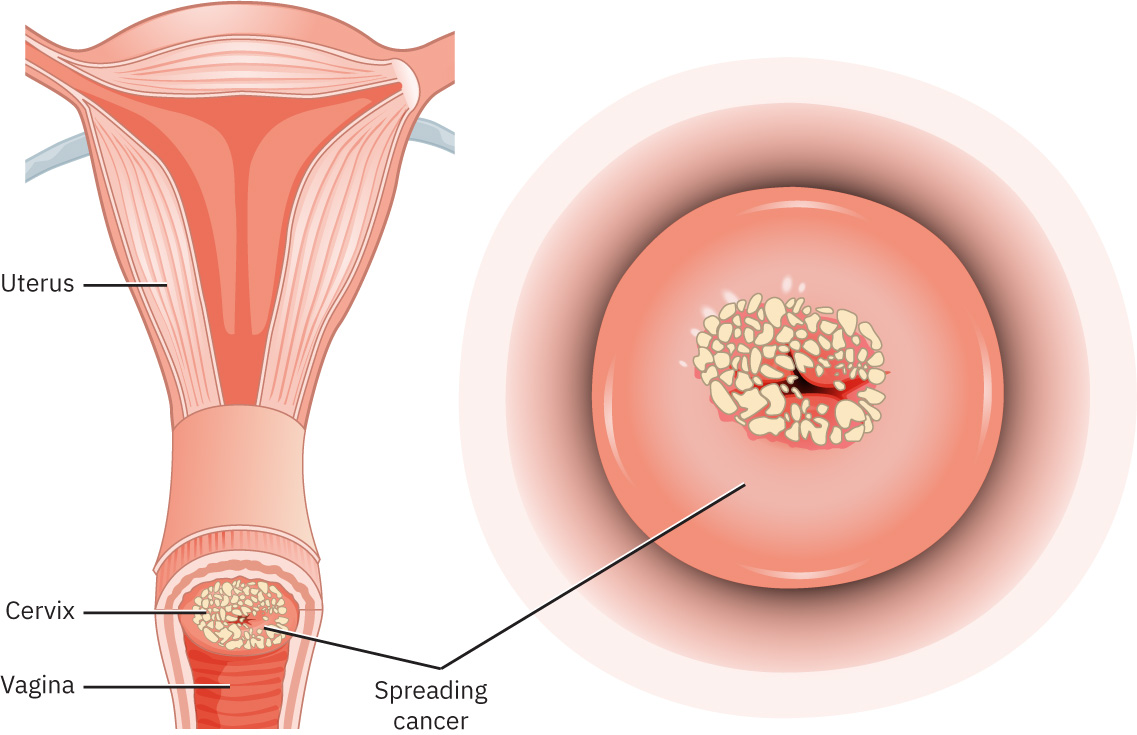 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.6.4.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.6.4.
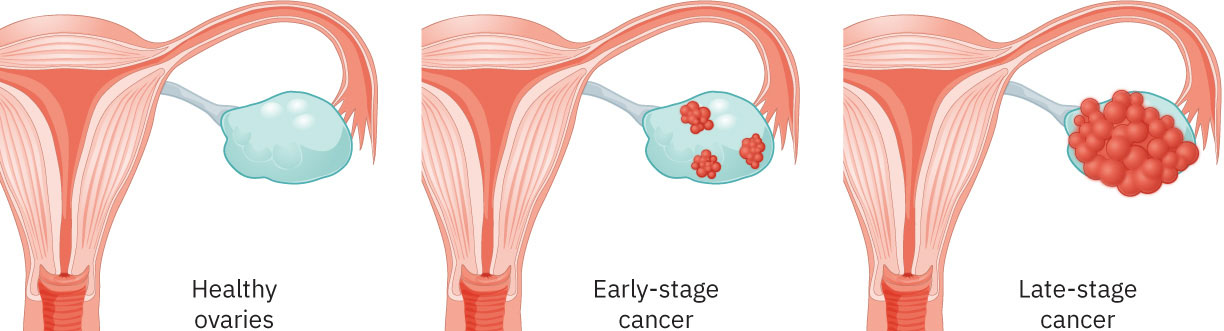 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.6.4.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.6.4.
Nursing Assessment
NCLEX Focus
Prioritize high-risk symptom recognition (postcoital or postmenopausal bleeding, persistent pelvic pain, unexplained weight loss) and timely diagnostic follow-through.
- Assess screening history (Pap/HPV co-testing and prior abnormal results).
- Verify age- and surgery-context screening applicability (for example no routine cervical screening before age 21 and individualized discontinuation decisions after 65 or after hysterectomy when criteria are met).
- Evaluate red-flag symptoms: abnormal bleeding, persistent discharge, pelvic pressure/pain, nonhealing vulvar lesions.
- For vulvar/vaginal-risk concern, assess persistent itching or burning, nonhealing sore, wart-like growth, raised/discolored vulvar skin, changing mole, or groin-node swelling.
- If cervical screening is abnormal, anticipate ASCCP/Bethesda-guided stratification steps and confirm follow-up colposcopy/biopsy plans.
- For ovarian-risk concern, assess persistent bloating, early satiety, urinary urgency/frequency, and unexplained bowel-pattern change.
- Include ovarian-risk profile cues such as obesity, nulliparity, infertility, endometriosis history, and longer lifetime estrogen exposure patterns.
- Include cancer-site specific red flags: new breast/axillary lump or nipple change, postmenopausal bleeding, and persistent pelvic fullness/bloating.
- Collect risk-profile cues (HPV exposure, smoking, immunocompromise, family/genetic risk factors).
- For endometrial-risk contexts, assess obesity, PCOS history, and prolonged unopposed-estrogen exposure patterns.
- Assess treatment readiness, understanding of diagnostic steps, and psychosocial distress burden.
- Monitor peri-procedural and treatment-related adverse effects (bleeding, infection, pain, fatigue).
Nursing Interventions
- Provide evidence-based education on cancer prevention, vaccination, and screening intervals.
- Clarify that professional organizations may differ on interval details; reinforce current local guideline use and shared decision-making when recommendations diverge.
- Prepare patients for diagnostic procedures (Pap/HPV testing, colposcopy, biopsy, imaging) and postprocedure expectations.
- Reinforce postprocedure expectations after colposcopy/LEEP/biopsy (possible light vaginal bleeding, peripad use, return precautions, and clear result-communication timeline).
- After endometrial/cervical biopsy, reinforce return precautions for heavy vaginal bleeding (for example soaking a pad about every 1 to 2 hours), fever, or worsening abdominal pain.
- In high-risk ovarian contexts, explain limitations of CA-125 and transvaginal ultrasound as stand-alone screening tests and reinforce individualized surveillance planning.
- Reinforce urgent return precautions for heavy bleeding, fever, severe pain, or worsening systemic symptoms.
- In pregnancy-associated cancer contexts, support informed discussions on treatment timing options, maternal-fetal implications, and ethical support resources.
- Coordinate interdisciplinary oncology care and supportive services for patient and family.
- Deliver trauma-informed, culturally sensitive communication during high-stress diagnosis and treatment decisions.
Vague-Symptom Dismissal
Treating persistent abnormal bleeding or pelvic symptoms as benign without timely workup can delay diagnosis to later-stage disease.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| breast-cancer-chemotherapy-safety-and-support (chemotherapy) | Site- and stage-specific regimens | Requires adverse-effect monitoring, infection-prevention teaching, and symptom escalation planning. |
| sexual-history-risk-linking-and-preventive-counseling (hpv-vaccine) | Cervical/vulvovaginal cancer-prevention contexts | Core prevention strategy; reinforce eligibility, schedule completion, and screening continuation. |
Clinical Judgment Application
Clinical Scenario
A postmenopausal patient reports intermittent bleeding and pelvic discomfort for 2 months but delayed care because symptoms were “probably stress-related.”
- Recognize Cues: Postmenopausal bleeding is a high-priority malignancy warning sign.
- Analyze Cues: Delay in evaluation increases risk of later-stage diagnosis.
- Prioritize Hypotheses: Immediate priority is endometrial/uterine pathology exclusion with expedited diagnostic workup.
- Generate Solutions: Arrange urgent gynecologic assessment, biopsy pathway, and symptom support.
- Take Action: Escalate for definitive testing and provide clear follow-up safety instructions.
- Evaluate Outcomes: Timely diagnosis is established and stage-appropriate treatment initiated.
Related Concepts
- benign-reproductive-growths - Benign and malignant bleeding or mass symptoms can overlap and require careful differentiation.
- structural-reproductive-disorders - Structural abnormalities may coexist and complicate diagnostic interpretation.
- functional-reproductive-disorders - Functional bleeding patterns must not obscure cancer warning signs.
- therapeutic-communication - Oncology conversations require clear, compassionate, and culturally safe communication.
- culturally-competent-care - Equitable cancer care depends on language access and context-sensitive counseling.
Self-Check
- Which symptoms in reproductive oncology should trigger urgent diagnostic escalation?
- Why does ovarian cancer frequently present at more advanced stages?
- How do nursing education and screening outreach improve gynecologic cancer outcomes?