Benign Reproductive Growths
Key Points
- Benign growths are noncancerous but can still cause bleeding, pain, pressure symptoms, fertility issues, and quality-of-life burden.
- Common entities include uterine fibroids, endometrial polyps, ovarian cysts, and benign cervical or vulvovaginal lesions.
- Many findings are incidental and monitored, while symptomatic or complicated cases require pharmacologic or surgical intervention.
- Nursing education on warning signs and follow-up timing is essential for safe management.
Pathophysiology
Benign growths arise from overgrowth of reproductive tissues without malignant invasion. Uterine leiomyomas (fibroids) originate from smooth muscle and are hormonally responsive, often regressing after menopause. Endometrial polyps arise from uterine lining proliferation and may cause irregular or heavy bleeding.
Ovarian cysts are fluid- or blood-containing sacs from ovarian tissues and are often asymptomatic, though rupture or torsion can cause acute pain and surgical urgency. Benign cervical and vulvovaginal lesions may present with bleeding, discomfort, irritation, or infection-like symptoms. For incidental ovarian-cyst findings, follow-up planning should align with structured ultrasound-risk guidance using menstrual/menopause status and family-history context.
Common functional ovarian cyst types include follicular cysts (often self-resolving over 1 to 3 months) and corpus luteum cysts, which may enlarge, bleed, or contribute to torsion risk. Surgical approach is often size/risk based, with laparoscopy favored for smaller likely-benign lesions and laparotomy considered for large or malignancy-suspicious cysts.
Clinical management balances symptom severity, reproductive goals, and risk profile. Observation is appropriate for many asymptomatic lesions; active treatment is used when pain, bleeding, mass effect, or complication risk increases.
For uterine fibroids, common symptom clusters include dysmenorrhea, menorrhagia/metrorrhagia, pelvic fullness, urinary frequency, dyspareunia, low-back pain, and fertility-related complications. Treatment can range from hormonal symptom control to procedure-based options such as myomectomy, hysterectomy, endometrial ablation, myolysis, and uterine-artery embolization.
Classification
- Uterine benign growths: Fibroids (leiomyomas) and endometrial polyps.
- Ovarian benign growths: Functional or other nonmalignant cystic lesions.
- Cervical benign growths: Incidental nonmalignant cervical lesions/cysts.
- Vulvovaginal benign growths: Cysts and localized noncancerous tissue proliferations.
Cervical Benign Growth Highlights
- Benign cervical growths are often incidental exam findings but may present with minor postcoital bleeding.
- Nabothian (mucous) cysts usually require no treatment unless very large or symptomatic.
- Cervical polyps are typically fleshy red protrusions and are often observed unless bothersome to the patient.
- HPV-related genital warts can involve cervix, vagina, vulva, or perianal tissue; treatment may include provider-applied acidic therapy or surgical removal in severe/abnormal-cell cases.
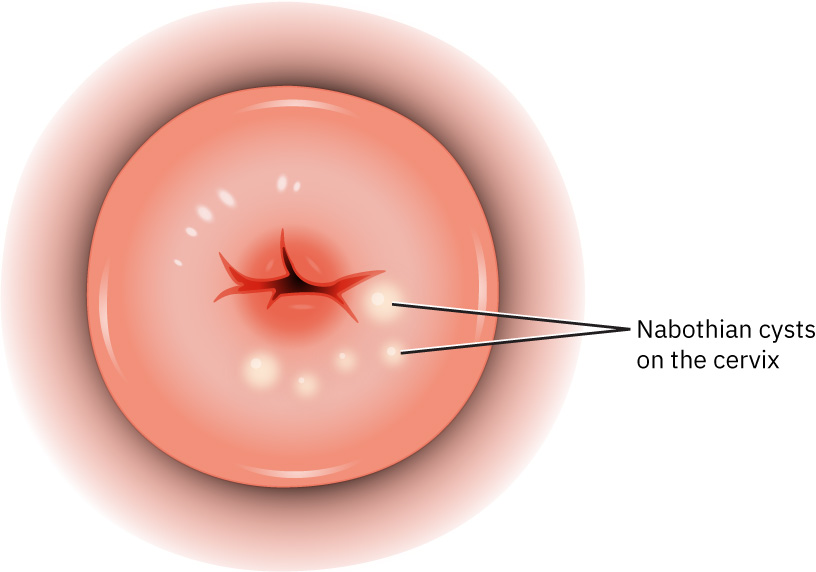 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.6.3.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.6.3.
Vulvar Benign Growth Highlights
- Bartholin-cyst formation commonly reflects obstruction of a Bartholin gland duct and can progress from painless swelling to painful infection.
- Initial conservative care includes warm compresses or sitz baths to support drainage and symptom resolution.
- Infected cysts may involve organisms such as E. coli, MRSA, and pathogens associated with gonorrhea/chlamydia exposure.
- Severe inflammation or abscess presentation may require incision and drainage.
Nursing Assessment
NCLEX Focus
Prioritize bleeding pattern changes, pain severity, and signs of acute complications such as torsion or significant blood loss.
- Assess menstrual changes (heavy flow, irregular bleeding, postcoital bleeding, postmenopausal bleeding).
- When postcoital bleeding is present, include focused cervical lesion assessment (cyst, polyp, wart pattern) and follow-up plan.
- Evaluate pelvic pain, pressure, urinary frequency, bowel symptoms, and dyspareunia.
- For vulvar masses, assess for unilateral tender swelling near the vaginal opening, progressive pain, erythema, fever, or drainage suggesting infected Bartholin cyst/abscess.
- Screen for acute red flags: sudden severe unilateral pain, fever, syncope, or heavy bleeding.
- Clarify fertility goals and symptom impact on daily functioning.
- Track imaging and follow-up intervals based on menopause status and risk profile.
Nursing Interventions
- Explain diagnosis and expected natural history (for example fibroid stability/regression patterns).
- Reinforce medication teaching for bleeding or pain control, including use timing and side-effect monitoring.
- Prepare and support patients during diagnostic procedures (ultrasound, office evaluations, biopsy when indicated).
- Match procedure counseling to reproductive goals (for example uterus-preserving myomectomy versus definitive hysterectomy; discuss fertility impact after endometrial ablation).
- Educate on when to seek urgent care for possible torsion, rupture, or hemorrhage.
- Teach vulvar-cyst self-care and return precautions: escalating pain, fever, worsening swelling, or persistent symptoms despite conservative measures.
- Coordinate specialist referral for persistent symptoms, fertility concerns, or surgical planning.
Postmenopausal-Bleeding Rule
Any postmenopausal uterine bleeding requires prompt evaluation, even when benign causes are suspected.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| antifibrinolytics (tranexamic-acid) | Heavy-bleeding control contexts | Used for menorrhagia reduction; teach cycle timing and thrombosis warning signs. |
| levonorgestrel-intrauterine-system | Fibroid/polyp bleeding-management contexts | May reduce heavy bleeding in selected benign-growth presentations. |
Clinical Judgment Application
Clinical Scenario
A perimenopausal patient presents with progressively heavy bleeding, pelvic pressure, fatigue, and intermittent sharp unilateral pelvic pain.
- Recognize Cues: Pattern suggests symptomatic uterine growths with possible intermittent ovarian complication.
- Analyze Cues: Combined bleeding burden and pain create anemia and acute-event risk.
- Prioritize Hypotheses: Priority is hemodynamic safety and urgent exclusion of ovarian torsion/rupture.
- Generate Solutions: Initiate bleeding/pain assessment, imaging coordination, and expedited gynecologic review.
- Take Action: Escalate acute symptoms, implement supportive care, and reinforce follow-up plan.
- Evaluate Outcomes: Complications are excluded or treated, and long-term symptom management is established.
Related Concepts
- ovarian-cysts - Dedicated concept note for ovarian-cyst classification, complication recognition, and urgent escalation pathways.
- fibroids - Dedicated concept note for fibroid symptom patterns, fertility-centered treatment pathways, and escalation planning.
- endometrial-polyps - Dedicated concept note for endometrial-polyp diagnosis and management pathways.
- abnormal-uterine-bleeding - Heavy or irregular bleeding from benign growths often enters care through AUB evaluation pathways.
- functional-reproductive-disorders - Functional and benign structural conditions often overlap clinically.
- structural-reproductive-disorders - Structural changes can coexist with benign growth patterns.
- causes-of-infertility - Benign uterine/ovarian conditions can interfere with conception and implantation.
- preconceptual-care - Early management can improve reproductive planning outcomes.
- therapeutic-communication - Sensitive bleeding and sexual-function symptoms need supportive communication.
Self-Check
- Which benign-growth symptoms require urgent rather than routine follow-up?
- Why does menopausal status change management of polyps and bleeding?
- How do fertility goals influence treatment selection for fibroids and ovarian cysts?