Structural Reproductive Disorders
Key Points
- Structural reproductive disorders may be acquired (for example pelvic floor prolapse and fistula) or congenital (Mullerian malformations).
- Symptoms often include pelvic pressure, incontinence, constipation, pain, and reproductive complications.
- Accurate assessment requires symptom history, pelvic examination, and selected imaging or procedural diagnostics.
- Nursing care combines education, symptom support, risk-factor modification, and timely escalation to surgical teams when needed.
Pathophysiology
Structural disorders reflect weakened support tissues, abnormal organ relationships, or embryologic formation differences that alter normal pelvic and reproductive function. Pelvic floor weakness can lead to prolapse syndromes (cystocele, rectocele, uterine prolapse) with urinary, bowel, and pressure symptoms. Vaginal fistulas create abnormal communications between vagina and urinary or gastrointestinal structures, causing persistent leakage and infection risk.
For reproductive fistulas, common acquired etiologies include obstetrical trauma from childbirth, operative vaginal delivery, and perineal surgical repair contexts (for example episiotomy or laceration repair). Other causes include gynecologic surgical injury, congenital malformation pathways, and female genital mutilation (FGM) injury. Global burden is highest where prolonged obstructed labor and limited surgical access delay definitive obstetric care.
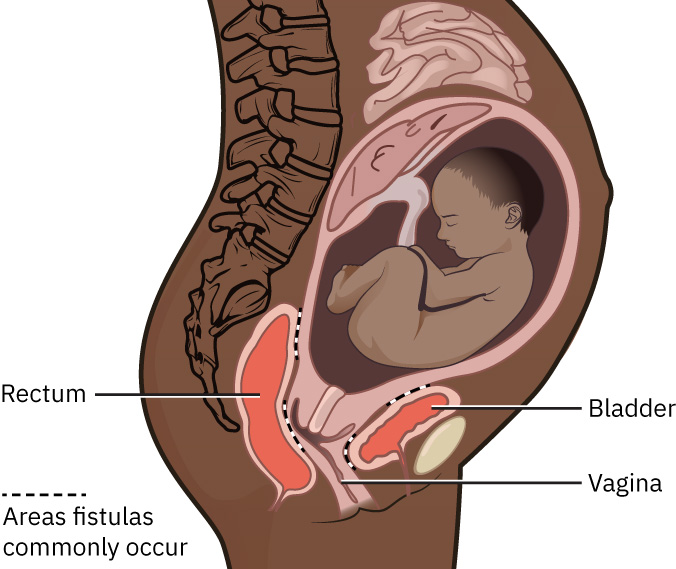 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.6.2.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.6.2.
Uterine prolapse, cystocele (anterior vaginal prolapse), and rectocele (posterior vaginal prolapse) are common postmenopausal and parity-associated patterns, and procedural management may be required when conservative support is insufficient.
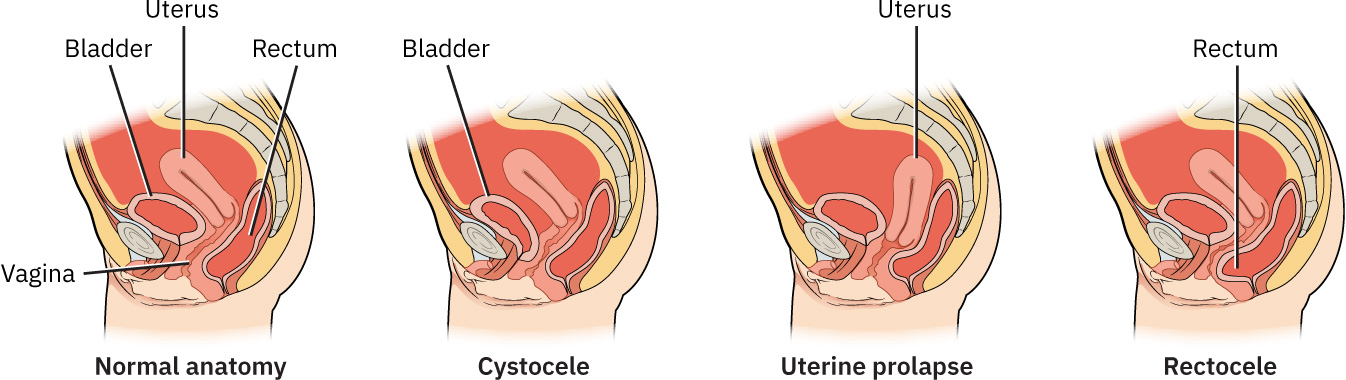 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.6.2.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.6.2.
Important risk factors for pelvic-floor disorders include pregnancy, vaginal birth, higher parity, connective-tissue disorders, obesity, chronic constipation, chronic cough, and hysterectomy history. Symptom burden can reduce quality of life and may lead to avoidance of social or sexual activity. Underdiagnosis is common because some patients avoid disclosure due to embarrassment or assume symptoms are normal aging.
Congenital malformations of reproductive structures (Mullerian anomalies) arise from disrupted embryonic duct development and can present later through infertility, miscarriage, ectopic pregnancy, dyspareunia, or chronic pelvic pain. These abnormalities may remain undiagnosed until reproductive evaluation occurs and are commonly confirmed with pelvic examination, ultrasound, or selected surgical assessment. Vaginal septum variants are one structural presentation that may first appear as painful penetration attempts or obstructed menstrual outflow with cyclic pain; associated urinary or uterine anomalies should be considered during comprehensive evaluation.
Management depends on severity and patient goals. Conservative approaches include pelvic floor therapy, pessary use, and risk-factor modification; definitive treatment may require surgical repair or reconstruction.
Classification
- Pelvic support disorders: Cystocele, rectocele, and uterine prolapse.
- Abnormal-connection disorders: Rectovaginal, vesicovaginal, and urethrovaginal fistulas.
- Broad vaginal-fistula category: Vaginal communication with adjacent urinary or gastrointestinal structures.
- Congenital malformation disorders: Uterine and vaginal developmental anomalies (Mullerian spectrum).
- Impact domains: Urinary function, bowel function, sexual comfort, fertility, and psychosocial health.
Nursing Assessment
NCLEX Focus
Prioritize symptom impact on continence, infection risk, and quality of life while screening for complications that need urgent evaluation.
- Assess pelvic pressure, bulge sensation, urinary/stool leakage, constipation, and pain patterns.
- Characterize prolapse-pattern cues: anterior vaginal pressure/urinary retention or urgency-frequency (cystocele), stool trapping/defecation difficulty (rectocele), and vaginal bulge/fullness with incontinence (uterine prolapse).
- Screen for recurrent urinary or vaginal infections and foul discharge suggestive of fistula.
- In suspected reproductive fistula, ask specifically about urine or stool leakage from the vagina and persistent foul odor.
- Collect obstetric, surgical, and trauma history, including prolonged labor or operative birth risk factors.
- Ask sensitively about prior genital cutting or scar history when FGM-related injury risk is clinically relevant.
- Assess barriers to disclosure (embarrassment, stigma, or belief that symptoms are expected with aging) that may delay diagnosis.
- Evaluate fertility history and recurrent pregnancy-loss patterns suggestive of congenital anomalies.
- In suspected vaginal septum, assess penetrative pain history and signs of menstrual outflow obstruction and coordinate urogynecologic evaluation.
- Use validated symptom tools (pelvic floor questionnaires) when available to track severity over time.
- Confirm infection-rule-out testing is completed (for example UTI or related infection evaluation) before assigning primarily functional pelvic-floor diagnosis.
- For moderate-to-severe symptom burden, prepare for additional diagnostics such as cystoscopy, urodynamics, or colonoscopy when ordered.
Nursing Interventions
- Educate on condition mechanism and realistic conservative-versus-surgical treatment expectations.
- Reinforce pelvic floor strengthening, bladder/bowel training, and modifiable risk management.
- Provide postoperative and device-use guidance when pessary or surgical interventions are used.
- Reinforce common management pathways for pelvic organ prolapse: Kegel-based strengthening, selected hormone-therapy support, pessary fitting, and surgical repair when conservative measures are insufficient.
- For pessary users, teach wear-and-care routine: many can be worn for several days (including during intercourse), then removed and cleaned with soap and water before reinsertion.
- Clarify follow-up options for pessary care (self-removal/reinsertion versus scheduled office maintenance visits based on patient ability and plan).
- Teach expected device side effects (increased vaginal discharge or odor) and comfort measures, including vaginal-gel options when appropriate.
- For menopausal patients using pessaries, reinforce estrogen-cream support when prescribed for vaginal irritation.
- Explain that very small fistulas may occasionally heal spontaneously, but most symptomatic reproductive fistulas require surgical repair.
- Promote early reporting of infection signs, escalating pain, heavy bleeding, or severe functional decline.
- Offer culturally safe care and trauma-informed communication for patients with high-stigma etiologies.
- For FGM-related injury, use survivor-centered counseling and coordinated referral pathways that address both physical and psychosocial recovery needs.
- Reinforce that selected congenital vaginal septa can be corrected with targeted surgical procedures when symptoms or outflow obstruction are present.
- Normalize treatment-seeking and proactively address stigma so patients report continence, bowel, and prolapse symptoms earlier.
Silent-Progression Risk
Delayed care for prolapse or fistula symptoms can worsen continence, infection burden, and psychosocial distress.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| vaginal-infections-and-other-conditions (topical-vaginal-estrogen) | Local estrogen contexts | May support tissue integrity in selected prolapse-management plans when appropriate. |
| antibiotics | UTI or vaginal infection treatment contexts | Essential when structural disorders produce recurrent or persistent infection patterns. |
Clinical Judgment Application
Clinical Scenario
A postpartum patient reports persistent urine leakage from the vagina, foul odor, and recurrent urinary infections after prolonged labor and operative delivery.
- Recognize Cues: Pattern suggests possible vesicovaginal fistula rather than routine postpartum incontinence.
- Analyze Cues: Ongoing leakage and infection indicate structural communication requiring specialist evaluation.
- Prioritize Hypotheses: Priority is fistula diagnosis confirmation and infection control.
- Generate Solutions: Arrange urgent gynecologic/urogynecologic evaluation and interim symptom/infection management.
- Take Action: Escalate promptly, provide supportive counseling, and coordinate multidisciplinary follow-up.
- Evaluate Outcomes: Diagnosis is clarified, complications are treated, and definitive repair planning is established.
Related Concepts
- functional-reproductive-disorders - Functional and structural disorders often coexist and complicate symptom interpretation.
- fertility-and-conception - Structural abnormalities can impair gamete transport and implantation.
- causes-of-infertility - Congenital and acquired pelvic structural causes are major infertility contributors.
- preconceptual-care - Early identification of structural risk can improve pregnancy planning safety.
- therapeutic-communication - Sensitive symptoms require trust-building and nonjudgmental care.
Self-Check
- Which findings distinguish pelvic floor prolapse from fistula-related leakage?
- Why do some congenital malformations present only when fertility is evaluated?
- Which symptoms in structural disorders require immediate specialist escalation?