Fertility and Conception
Key Points
- Fertility requires viable gametes, accurate timing, and a hormonally receptive endometrium.
- Conception depends on coordinated ovulation, fertilization in the fallopian tube, and successful implantation in the uterus.
- Egg viability is brief (about 12 to 24 hours), whereas sperm may survive up to 5 days in the female tract.
- The fertile window starts up to about 1 week before ovulation and extends through the day after ovulation.
- Age-related fecundity decline and psychosocial stressors can reduce conception probability and influence care needs.
Pathophysiology
Fertility is the capacity to conceive, while infertility commonly refers to no conception after 12 months of regular unprotected intercourse or after 6 months when the female partner is older than 35 years. Definitions may also include inability to carry a pregnancy to live birth. Global burden is high, with about one in six people of reproductive age affected during their lifetime. In natural conception, cycle-level success is limited even in healthy couples, often estimated at roughly 20 to 37 percent per cycle. The section emphasizes three required conditions for conception: release of an egg, presence of viable sperm, and a uterus/endometrium prepared for implantation. Environmental exposures, infections, genetics, and substance use can disrupt any of these requirements.
Behavioral exposures affect fertility in both partners: tobacco can reduce hormone production and impair sperm DNA quality, and ongoing alcohol or drug use can reduce ovulatory and sperm-function reliability.
Ovulation begins with follicle-stimulating hormone (FSH) driven follicular development and rising estradiol, followed by a luteinizing hormone (LH) surge that releases the mature ovum. The ovum is captured by fimbriae and moved through the fallopian tube by cilia and peristalsis. Fertilization typically occurs in the ampulla; after one sperm penetrates, the zona pellucida becomes resistant to additional sperm. A normally formed zygote contains forty-six chromosomes, with twenty-three contributed by each gamete.
Cycle physiology follows phased hormonal patterns: follicular (endometrial proliferation and dominant follicle selection), ovulatory (LH surge with ovum release, often around mid-cycle), and luteal (corpus luteum progesterone secretion supporting implantation readiness). Rising progesterone in the luteal phase also contributes to basal body temperature elevation used in fertility tracking.
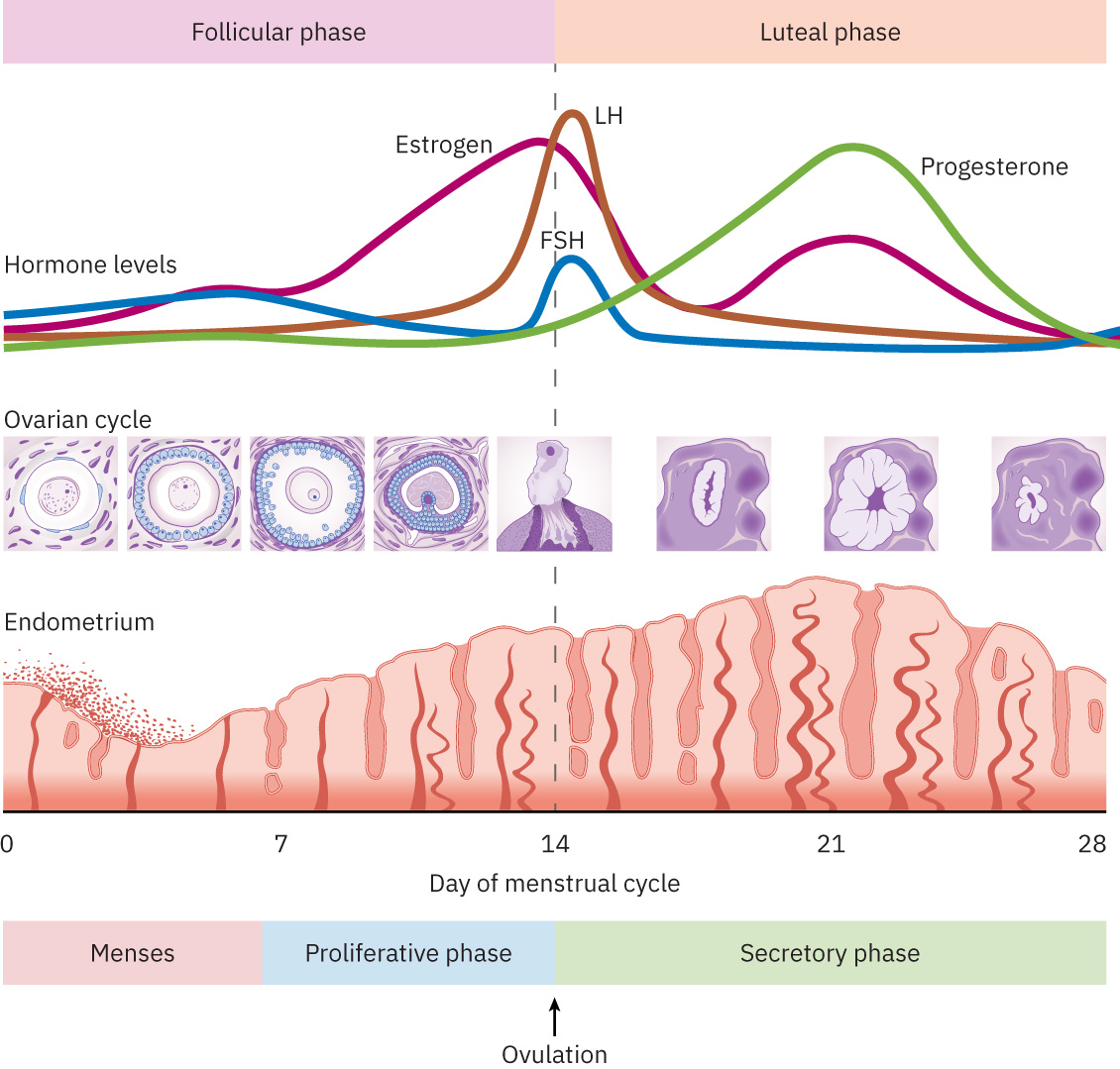 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.3.3.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.3.3.
On the male side of conception physiology, sperm develop in seminiferous tubules and then mature in the epididymis (about 12 days on average) before ejaculation. Each ejaculation can release up to about 200 million sperm, but sperm are only a small fraction of ejaculate volume; most semen volume comes from accessory-gland secretions, which support transport and viability. After vaginal deposition, sperm movement depends on flagellar propulsion plus reproductive-tract contractions that help transport sperm through the cervix toward the upper tract.
Spermatogenesis requires a temperature about 2 to 3 C below core body temperature, occurs continuously after puberty, and takes roughly 64 days per production cycle. Daily production is high, but sperm counts tend to decline gradually with age after the mid-30s.
After fertilization, the zygote undergoes mitotic divisions (2-, 4-, 8-, and 16-cell stages) to form a morula in about 4 days, then becomes a blastocyst around day 5. During this interval it continues tubal transport toward the uterus; implantation often begins about 5 to 6 days after fertilization, most commonly in the fundal endometrium, with trophoblast invasion initiating early placental development.
Population-level conception probability declines with female age. Approximate 1-year conception rates are about 85% below age 30, 75% at age 30, 66% at age 35, and 44% at age 40.
Classification
- Gamete factors: Oocyte maturation/ovulation quality and sperm production, maturation, motility, and viability.
- Transport/timing factors: Coordinated ovulation timing, sperm migration, and tubal transport.
- Cycle-phase factors: Follicular development, ovulatory LH surge, luteal progesterone support, and predictable fertile-window cues (for example egg-white cervical mucus before ovulation).
- Uterine factors: Endometrial proliferation/secretory transformation and implantation receptivity.
- Psychosocial and population factors: Stress, social pressure, delayed childbearing, and fertility-knowledge gaps (including overestimation of assisted-reproduction success at advanced age).
Nursing Assessment
NCLEX Focus
Priority items often test whether conception barriers are primarily ovulatory, sperm-related, timing-related, uterine/implantation-related, or psychosocial.
- Assess menstrual and ovulatory history, including cycle regularity and signs of ovulation.
- Review potential fertility disruptors: substance use, environmental exposures, chronic conditions, and infection risk.
- Elicit timing history (intercourse relative to ovulation) and prior duration of conception attempts.
- Screen psychosocial burden (stress, stigma, relationship strain, financial barriers) and fertility-literacy gaps.
- Assess beliefs driving delayed childbearing decisions (for example partnership timing, career/education demands, or assumptions about future assisted-reproduction options).
- Identify age-related risk context and understanding of fecundity decline over time.
Nursing Interventions
- Provide clear education on conception timing windows, including short ovum viability and longer sperm survival.
- Counsel couples to have intercourse at least every other day during the fertile window (up to about 1 week before ovulation through the day after ovulation).
- Teach physiologic conception sequence (ovulation → fertilization → implantation) to support informed planning.
- Reinforce preconception risk reduction (substance cessation, environmental safety, and health optimization).
- Counsel both partners on smoking cessation and alcohol/drug reduction before conception attempts to improve ovulatory and sperm quality outcomes.
- Offer stress-management resources such as mindfulness groups or cognitive-behavioral therapy referral when infertility stress is high.
- Teach lubricant safety when trying to conceive: avoid saliva, olive/coconut oil, and nonfertility lubricants that may impair sperm function.
- Clarify that coital position has no evidence-based effect on conception odds.
- Offer supportive counseling and normalize emotional responses to delayed conception or infertility concerns.
- Provide explicit age-related fertility education to both partners and correct misconceptions that assisted reproductive technologies can fully offset delayed childbearing.
- Coordinate timely referral to reproductive specialists when infertility criteria are met or risk factors are known.
Timing-Only Assumption
Assuming delayed conception is only a timing issue can postpone evaluation of endocrine, sperm, tubal, uterine, or psychosocial contributors.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| treating-infertility (gonadotropins) | FSH and related ovulation-induction agents | Used in fertility treatment pathways; requires cycle monitoring and patient education on timing. |
| treating-infertility (progesterone-therapy) | Luteal support regimens | Supports endometrial receptivity in selected treatment plans and early pregnancy contexts. |
Clinical Judgment Application
Clinical Scenario
A 36-year-old patient reports 12 months of unsuccessful attempts to conceive, irregular cycle signs, and high stress related to work and family expectations.
- Recognize Cues: Age-related decline risk, possible ovulatory irregularity, and psychosocial strain are all present.
- Analyze Cues: Conception barriers may be multifactorial rather than a single timing problem.
- Prioritize Hypotheses: Priority hypothesis is combined ovulatory/timing challenge with psychosocial burden affecting fertility planning.
- Generate Solutions: Provide cycle-timing education, psychosocial support, risk-factor review, and referral planning.
- Take Action: Initiate education, document infertility-duration criteria, and coordinate specialist follow-up.
- Evaluate Outcomes: Patient demonstrates understanding of conception physiology and engages in an evidence-based care plan.
Related Concepts
- preconceptual-care - Preconception risk optimization improves fertility conditions before conception attempts.
- health-promotion-across-the-reproductive-lifespan - Fertility planning is a core reproductive-health promotion domain.
- reproductive-system - Hormonal and anatomic reproductive functions underpin conception physiology.
- family-health-and-cultural-factors - Family and cultural context shapes fertility decisions and stress experiences.
- culturally-competent-care - Fertility counseling is more effective when communication is culturally responsive.
Self-Check
- Why can conception fail even when intercourse appears well timed?
- Which timing facts about ovum and sperm viability are most clinically relevant for fertility counseling?
- When should nursing care escalate from education to formal infertility referral pathways?