Basic Terms of Fetal Heart Rate and Contraction Patterns
Pathophysiology
FHR patterns reflect fetal oxygenation, autonomic balance, and response to uterine activity. Contraction patterns influence uteroplacental perfusion and therefore fetal status. Sympathetic tone tends to raise FHR, parasympathetic tone lowers it, and hypoxia/hypercapnia-associated chemoreceptor activation can shift pattern behavior.
Classification
- Baseline: Normal is 110 to 160 bpm averaged over 10 minutes, reported in 5-bpm increments and calculated while excluding periodic changes and marked variability. Tachycardia is more than 160 bpm for 10 minutes; bradycardia is less than 110 bpm for 10 minutes.
- Variability: Minimal (5 bpm or less), moderate (6 to 25 bpm), marked (more than 25 bpm), or absent; variability reflects CNS-autonomic integrity and acid-base adaptation. Minimal variability can occur with acidemia concern but is not a stand-alone diagnosis of fetal compromise.
- Accelerations: Abrupt rises (onset-to-peak under 30 seconds) that are at least 15 bpm above baseline for at least 15 seconds and less than 2 minutes at or beyond 32 weeks; before 32 weeks, 10 bpm for 10 seconds is expected. Accelerations are generally reassuring.
- Decelerations: Early (gradual mirror pattern with contractions, commonly head-compression vagal response and usually benign), late (onset with contraction and recovery after contraction ends, with nadir after contraction peak), variable (abrupt declines, commonly at least 15 bpm below baseline for at least 15 seconds, usually cord-compression related, and not necessarily contraction-linked), prolonged (isolated decline of at least 15 bpm lasting 2 to 10 minutes).
- Uterine activity: Adequate pattern is generally 5 or fewer contractions in 10 minutes, with many contractions lasting about 45 to 60 seconds (sometimes up to about 90 seconds near second stage); tachysystole is more than 5 in 10 minutes across at least two consecutive intervals or prolonged contraction burden around 2 minutes or longer.
- Contraction terms: Frequency is start-to-start timing, duration is start-to-end seconds, and intensity is contraction strength.
- Strip scale orientation: Darker vertical lines usually indicate 1 minute and lighter lines 10-second intervals; FHR horizontal scale often uses 10-bpm steps and uterine-pressure scale commonly uses 5 to 10 mm Hg steps.
- Category system: Category I reassuring, Category II indeterminate, Category III abnormal and high risk; NICHD three-tier terminology supports more consistent interpretation and team communication. Category I commonly shows moderate variability with no concerning deceleration pattern and may include accelerations. Category II often includes intermediate findings such as minimal variability that warrant continued reassessment.
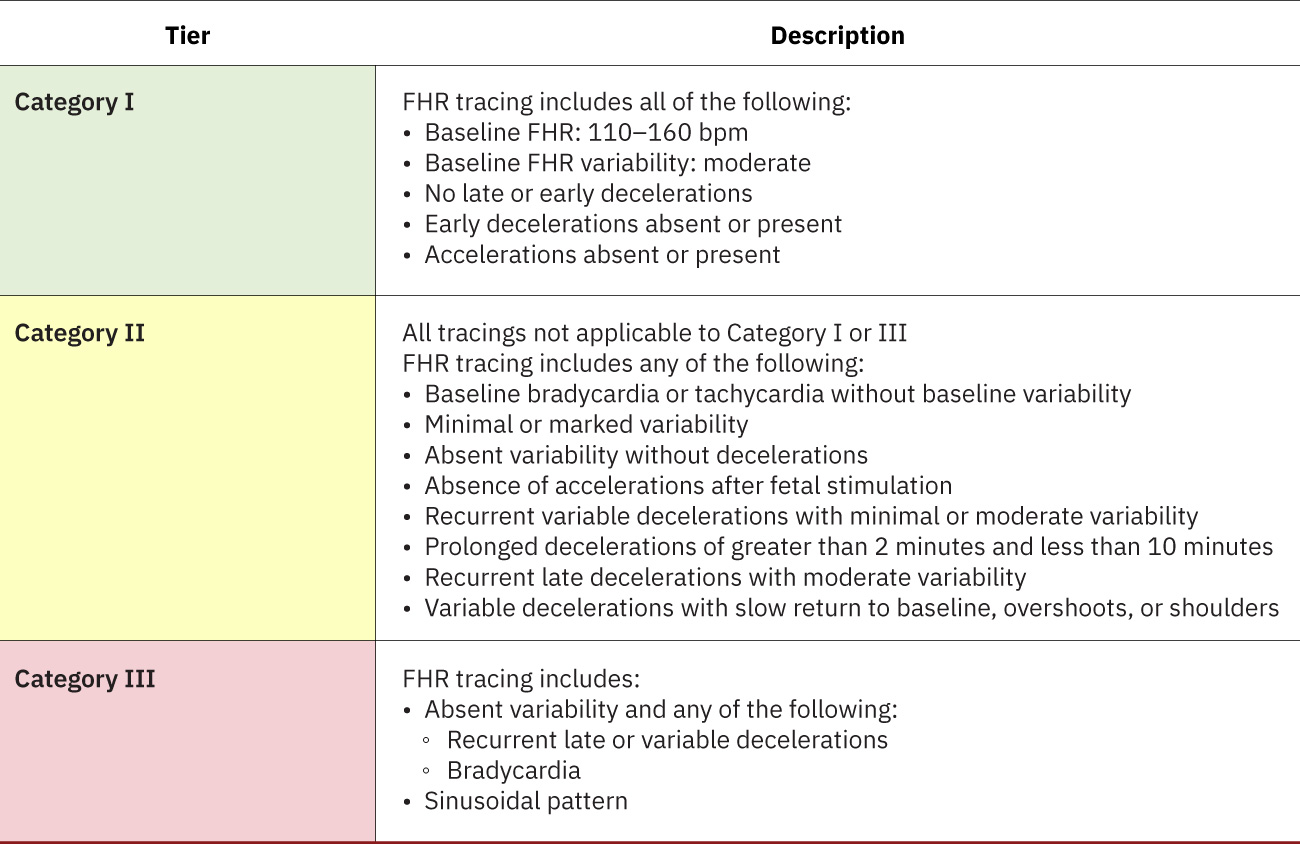 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.2.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.2.
- Sinusoidal pattern: Smooth regular wave (about 3 to 5 cycles per minute) with absent true variability, often associated with severe fetal compromise (for example anemia/blood-loss contexts).
Common baseline-rate risk contexts:
- Tachycardia contributors (maternal): Fever/infection, anxiety, dehydration, nicotine exposure, hyperthyroid state, and selected medications (for example atropine or terbutaline context).
- Tachycardia contributors (fetal): Hypoxia/compromise, infection, anemia, prematurity, or arrhythmia.
- Bradycardia contributors (maternal): Hypotension, neuraxial/anesthesia effects, hypoglycemia, hypothermia, selected medications (for example magnesium sulfate or beta-blocker exposure), major obstetric emergencies (for example abruption or uterine rupture), thyroid dysfunction, or monitor confusion with maternal pulse.
- Bradycardia contributors (fetal): Head-compression context, congenital heart block, hypoxia, and prolonged cord compression.
Nursing Assessment
- Identify baseline, variability, accelerations, and deceleration type.
- Apply gestational-age aware acceleration thresholds (10x10 before 32 weeks; 15x15 at/after 32 weeks) when judging reassurance.
- Identify sinusoidal tracing morphology separately from variability categories because it signals high-risk compromise.
- When determining baseline, confirm the full 10-minute window and avoid including accelerations/decelerations or marked-variability episodes.
- Differentiate reassuring versus concerning patterns (tachycardia, bradycardia, prolonged/late/variable decelerations).
- For late decelerations, prioritize uteroplacental-insufficiency differential (tachysystole/oxytocin effect, neuraxial hypotension, hypertensive disease, placental pathology, maternal-fetal anemia contexts).
- For prolonged decelerations, assess high-risk causes (uterine hyperactivity, cord compression, hypotension, abruption, seizure, impending birth) and recognize that deeper/longer events carry higher hypoxia risk.
- For minimal variability, review reversible/nonhypoxic contexts (for example fetal sleep cycle, medication effects including magnesium exposure, and prematurity) while maintaining serial reassessment.
- Treat absent variability as high-risk until proven otherwise; worsening trend from moderate to minimal to absent requires rapid escalation and provider notification.
- For marked variability (more than 25 bpm), recognize that baseline determination may become difficult and evaluate promptly for hypoxia-linked stress patterns, especially during second-stage labor.
- Interpret baseline tachycardia in full context: maternal fever is a common reversible contributor, and isolated tachycardia without deceleration concern is not by itself proof of fetal distress.
- Distinguish sustained baseline bradycardia from prolonged deceleration episodes before concluding etiology and urgency.
- Verify fetal-versus-maternal rate source whenever bradycardia is suspected to avoid response delays from signal misidentification.
- Interpret uterine pattern: frequency, duration, intensity, and resting tone.
- Identify whether the tracing is Category I, II, or III as part of standardized interpretation.
- Correlate pattern changes with maternal condition and stage of labor.
Nursing Interventions
- Initiate prompt pattern-based reassessment and escalation for nonreassuring changes.
- Align intervention urgency to category trajectory: routine care for Category I, intensified surveillance/reassessment for Category II, and immediate escalation for Category III.
- For fetal bradycardia concern, start immediate first-line sequence: maternal repositioning, IV fluid bolus when indicated, and urgent provider notification with trend summary.
- If bradycardia is associated with tachysystole and terbutaline is considered per order/policy, assess maternal pulse first and withhold when pulse is above 120 bpm.
- Document standardized interpretation and response plan, including monitoring method and category.
- Communicate findings clearly to team and patient/family.