Autonomic Nervous System Receptors and Drug Effects
Key Points
- The nervous system divides into central and peripheral components; the autonomic branch regulates involuntary organ responses.
- The ANS has two major divisions: sympathetic (fight-or-flight) and parasympathetic (rest-and-digest).
- Sympathetic pathways are linked to alpha and beta receptor families.
- Parasympathetic pathways are linked to nicotinic and muscarinic cholinergic receptors.
- Drug effects in ANS pharmacology depend on which receptor is stimulated or blocked.
- Homeostasis depends on dynamic SNS-PNS balance at target organs.
- Preganglionic signaling uses acetylcholine at nicotinic receptors in both SNS and PNS, while many drugs target postganglionic pathways for organ-selective effects.
- Core ANS drug groupings include cholinomimetic/cholinesterase-inhibiting pathways, anticholinergics, sympathomimetics, and adrenergic antagonists.
System Overview
The central nervous system (brain and spinal cord) integrates input, while the peripheral nervous system carries sensory and motor signaling between central structures and body organs. Motor output includes the somatic branch (voluntary skeletal-muscle movement) and autonomic branch (involuntary organ regulation).
ANS Divisions and Receptors
- Sympathetic nervous system (SNS): Associated with stress-response activation; key receptor families are alpha-adrenergic and beta-adrenergic.
- Parasympathetic nervous system (PNS): Associated with restorative organ activity; key receptor families are nicotinic and muscarinic cholinergic receptors.
Homeostasis Principle
Most target organs are regulated by relative SNS and PNS tone rather than by one branch alone. Clinical pharmacology decisions therefore focus on whether a drug mimics or blocks one side of this balance and what compensatory effects are expected in other organ systems.
Typical directional patterns include:
- SNS stimulation: Increased heart rate, increased blood pressure via vascular effects, and bronchodilation.
- PNS stimulation: Slower heart rate, relative blood-pressure lowering tendencies, bronchoconstriction, and increased digestive secretory/motility activity.
In threat-response physiology, catecholamines (epinephrine and norepinephrine) coordinate simultaneous multi-organ sympathetic activation to prioritize oxygen and glucose delivery to skeletal muscle. Excess sympathomimetic stimulation from substances such as heavy caffeine intake or cocaine can increase cardiac stress and worsen autonomic imbalance.
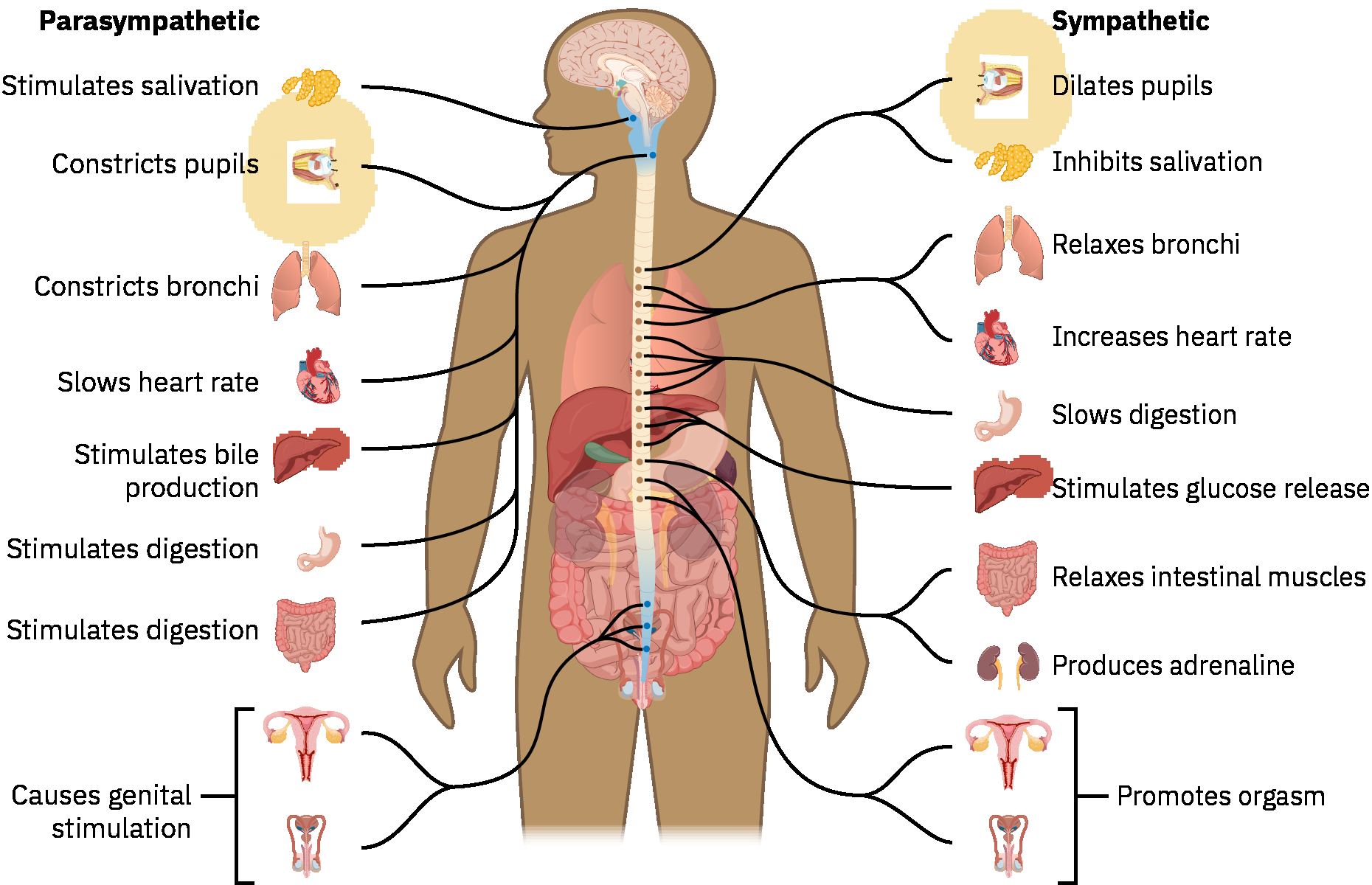 Illustration reference: OpenStax Pharmacology (autonomic system overview).
Illustration reference: OpenStax Pharmacology (autonomic system overview).
Neurotransmitter Pathway
- Preganglionic neurons: Release acetylcholine (ACh) onto nicotinic receptors.
- Postganglionic PNS neurons: Cholinergic; release ACh to target tissues.
- Postganglionic SNS neurons: Adrenergic; primarily release norepinephrine (with epinephrine as an additional adrenergic mediator).
Because preganglionic nicotinic signaling is shared across both branches, many clinical medications are designed to target postganglionic receptor systems for greater selectivity.
Adrenergic Receptor Subtypes
- Alpha-1
- Alpha-2
- Beta-1
- Beta-2
These subtype differences explain why autonomic medications can produce distinct organ effects even within the same sympathetic pathway.
Sympathetic Receptor Effect Patterns
| Receptor | Typical stimulation pattern | Typical inhibition pattern | Example context |
|---|---|---|---|
| Alpha-1 | Peripheral vasoconstriction, smooth-muscle contraction, pupil dilation | Vasodilation and smooth-muscle relaxation | Agonist: pseudoephedrine/phenylephrine; antagonist: tamsulosin |
| Alpha-2 | Reduced central sympathetic outflow | Limited direct clinical blockade role in this source context | Agonist: clonidine (antihypertensive/sedative context) |
| Beta-1 | Increased heart rate/contractility and increased renin release | Reduced heart rate and blood pressure | Agonist: dobutamine; antagonist: metoprolol |
| Beta-2 | Smooth-muscle relaxation, bronchodilation, selected vasodilation | Bronchoconstriction risk when blocked | Agonist: albuterol; nonselective blocker context: propranolol |
Agonist and Antagonist Framework
- Adrenergic agonists (sympathomimetics) mimic endogenous SNS stimulation.
- Adrenergic antagonists block SNS receptor effects.
- Dose-dependent dopamine effect in this source: can produce vasodilation in kidney, heart, and brain vascular beds depending on dosing range.
Beta-1 agonist cardiac effects are commonly described as:
- Positive chronotropic: increased heart rate
- Positive inotropic: increased contractile force
- Positive dromotropic: increased conduction speed (for example SA-to-AV node conduction)
Nonselective beta antagonism (beta-1 + beta-2 blockade) can inadvertently cause bronchoconstriction, so airway-risk assessment is necessary in asthma/COPD contexts.
Beta-2 agonist therapy can produce off-target effects, including tachycardia and hyperglycemia (via hepatic glycogenolysis), so glycemic and cardiovascular monitoring is relevant in susceptible patients.
Adrenergic Antagonist Highlights
- Alpha-1 antagonists: Promote vasodilation and smooth-muscle relaxation in lower urinary tract pathways.
- Example contexts: tamsulosin for improved urine flow with enlarged prostate, prazosin for blood-pressure reduction.
- Beta antagonists:
- Selective beta-blockers primarily inhibit beta-1 receptors (cardiac-focused effects).
- Nonselective beta-blockers inhibit beta-1 and beta-2 receptors (heart + lung effects), increasing bronchoconstriction risk in asthma/COPD.
- Clinical effect language commonly uses negative chronotropic, inotropic, and dromotropic patterns.
- Important nursing point: beta-blockers can mask hypoglycemia warning symptoms (for example tremor, tachycardia, nervousness).
Parasympathetic Pharmacology Highlights
- Cholinergics stimulate nicotinic or muscarinic receptors; most therapeutic designs in this source focus on muscarinic pathways.
- Nicotinic prototype context: Nicotine replacement (for example nicotine patch) acts as a nicotinic agonist in cessation pathways; direct nicotinic antagonism is not a routine clinical pathway in this source context.
- Muscarinic agonists (parasympathomimetics):
- Typical effects: smooth-muscle contraction, lower heart rate, bronchoconstriction, increased GI/GU tone, and pupillary constriction.
- Direct-acting examples: pilocarpine (glaucoma), bethanechol (urinary retention).
- Indirect-acting examples: pyridostigmine, physostigmine, donepezil.
- Muscarinic antagonists (anticholinergics/parasympatholytics):
- Inhibit ACh and shift tone toward sympathetic-dominant effects.
- Core mnemonic: SLUDGE (decreased salivation/lacrimation, urinary retention, drowsiness-dizziness, GI upset, blurred/dry eyes).
- Additional concerns: confusion and constipation, with heightened caution in older adults.
Applying the Nursing Process to ANS Medications
Assessment
- Anticipate cardio-respiratory monitoring (blood pressure, heart rate, lung sounds) because many ANS-active medications affect heart, lungs, and vascular tone.
- With anticholinergic pathways, monitor urinary retention, constipation, and dry-mouth symptoms.
- Screen for stimulant/substance exposure and unintended adrenergic triggers when sympathetic findings appear out of proportion to the clinical setting.
Planning
- Set adherence goals for medication-taking behavior.
- Define target vital-sign ranges aligned with indication.
- Verify patient teaching goals: mechanism, expected effects, and reportable adverse effects.
Implementation
- Use clear hold/administer parameters for ANS-active medications; if unclear, hold and clarify with provider per safe-medication policy.
- Source-specific default example for blood-pressure medication safety when no parameters are provided:
- hold if apical heart rate is below
60beats/minute and/or systolic blood pressure is below100mmHg.
- hold if apical heart rate is below
- Escalate marked vital-sign changes or suspected adverse effects promptly.
- Implement fall precautions when side-effect profile increases orthostasis/sedation/fall risk.
Evaluation
- Evaluate against the ordered therapeutic intent (for example improved urine flow or controlled heart rate/blood pressure).
- If benefit is not demonstrated, reassess risk-benefit balance and escalate for regimen review.
Prototype Pair Highlights by Receptor
- Nicotinic:
- Agonist example: nicotine-replacement therapy.
- Antagonist pathway: not clinically emphasized in this source.
- Muscarinic:
- Agonist example: pilocarpine.
- Antagonist example: atropine.
- Alpha-1:
- Agonist examples: pseudoephedrine, phenylephrine.
- Antagonist example: tamsulosin.
- Alpha-2:
- Agonist example: clonidine (including ADHD and hypertension contexts).
- Antagonist pathway: limited routine clinical use in this source.
- Beta-1:
- Agonist example: dobutamine.
- Antagonist example: metoprolol.
- Beta-2:
- Agonist example: albuterol.
- Antagonist example context: propranolol (nonselective blockade with bronchoconstriction risk).
Catecholamine examples (epinephrine and norepinephrine) can stimulate multiple adrenergic receptors simultaneously, supporting increased cardiac output and vasoconstrictive redistribution in high-acuity states.
Related Concepts
- neurological-system - CNS/PNS structure and autonomic control context.
- muscarinic-agonists - Pilocarpine-focused muscarinic agonist administration and DUMBBELSS monitoring.
- anticholinergics - Muscarinic antagonism and parasympatholytic effects.
- acetylcholinesterase-inhibitors - Indirect cholinergic augmentation pathway including donepezil context.
- alpha-2-agonists - Clonidine-centered central sympatholysis with rebound-hypertension precautions.
- beta-blockers - Beta-adrenergic antagonism in cardiovascular care.
- bronchodilators - Beta-2 and anticholinergic pathways in airway management.
- decongestants - Alpha-1 agonist nasal-vasoconstriction use and sympathomimetic safety cautions.
Self-Check
- Why does identifying receptor family matter before giving an autonomic medication?
- How do SNS and PNS balancing effects support homeostasis at one target organ?