Absorption — Pharmacokinetics
Key Points
- Absorption is the first ADME stage: drug travels from its administration site into systemic circulation.
- Common routes include oral, enteral, rectal, intranasal, inhalation, IM, SC, transdermal, and IV.
- The first-pass effect occurs with oral/enteral routes: GI enzymes and hepatic metabolism reduce the active drug that reaches circulation, lowering bioavailability.
- Alternate routes (transdermal, inhalation, injection, IV) bypass the first-pass effect.
- IV administration provides 100% bioavailability and the fastest onset; transdermal provides slow, steady delivery over extended periods.
- Life span differences significantly alter absorption — neonates have immature liver function (higher drug levels); older adults have reduced GI perfusion and subcutaneous fat (reduced absorption).
Pathophysiology
Absorption is the first stage of pharmacokinetics (ADME). After a drug is administered, it must travel from the site of entry into systemic circulation before distribution to target tissues can occur.
Drugs can enter the body through nine common routes:
- Oral (PO) — swallowed tablets or liquids
- Enteral — via GI tube (nasogastric, gastric, orogastric)
- Rectal — suppositories or enemas
- Intranasal — sprays into the nasal passages
- Inhalation — inhaled aerosols, vapors, or gases through the airway
- Intramuscular (IM) — injected into muscle tissue
- Subcutaneous (SC) — injected into subcutaneous tissue
- Transdermal — absorbed through the skin via patch or gel
- Intravenous (IV) — injected directly into a vein; bypasses absorption entirely
Classification
First-Pass Effect
When a drug is administered orally or enterally, absorption can be significantly reduced by two sequential processes:
- GI enzymes in the stomach and duodenum may deactivate protein-based drugs before they reach the intestine.
- Drug absorbed from the intestine enters the portal circulation and passes through the liver, where hepatic enzymes break down a portion of the drug before it reaches systemic circulation.
The fraction of drug that escapes into general circulation either binds to plasma proteins (inactive) or remains free to act at receptor sites. This process — the first-pass effect — reduces bioavailability (the percentage of the administered dose that reaches systemic circulation in active form). Multiple oral doses may be required before sufficient free drug accumulates to produce a therapeutic effect.
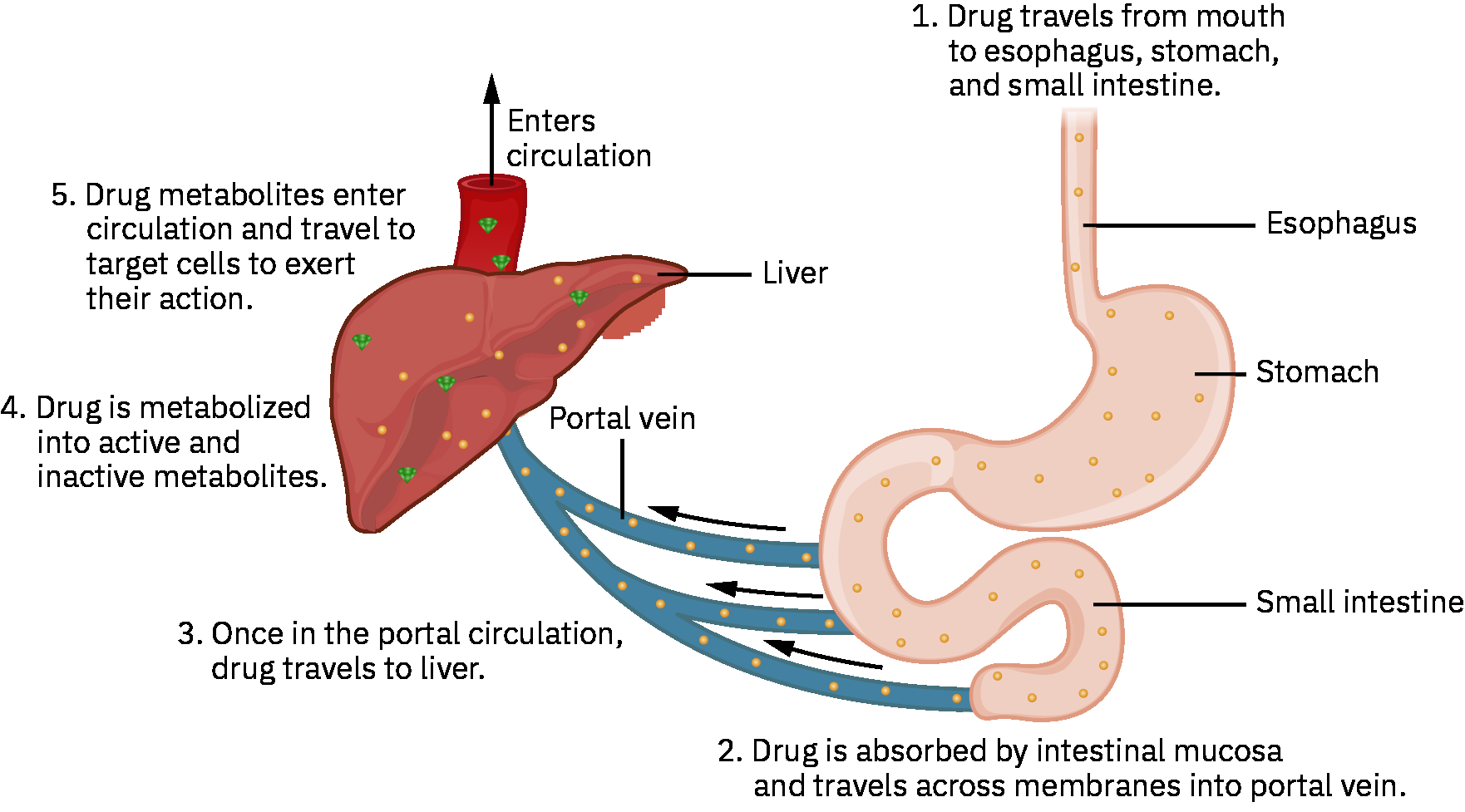 Illustration reference: OpenStax Pharmacology Ch.2.2.
Illustration reference: OpenStax Pharmacology Ch.2.2.
Alternate Routes (Bypassing First-Pass)
Routes that avoid the GI-hepatic pathway bypass the first-pass effect:
- Transdermal: Drug is absorbed through skin capillaries directly into systemic circulation, bypassing the liver. Provides slow, steady drug delivery — useful for extended symptom control. Only small drug molecules can cross the skin barrier. Examples: fentanyl (pain management), scopolamine (motion sickness), nitroglycerin (chronic angina prevention). Heat sources over patches accelerate absorption and risk toxicity.
- Inhalation: Drugs in gaseous, vaporized, or aerosol form absorb rapidly through lung tissue, bypassing the liver. Particle/droplet size determines depth of pulmonary tree penetration; smaller particles reach the alveoli. Bronchospasm can reduce inhalation depth and drug delivery.
- Injection (IM/SC): Drug enters the bloodstream via muscle or subcutaneous tissue capillaries without GI/hepatic passage. Drawbacks include pain, risk of infection from skin disruption, potential local side effects, and fluctuating drug levels.
- IV: Drug enters bloodstream directly with 100% bioavailability and immediate effect. Requires sterile technique; drug compatibility must be verified for co-infusions; risk of renal or hepatic toxicity exists.
Nursing Assessment
NCLEX Focus
Know which routes bypass the first-pass effect, what 100% bioavailability means clinically, and how life span factors alter absorption in neonates and older adults.
- Assess the prescribed administration route and confirm it is appropriate for the patient’s clinical status and the drug’s pharmacokinetic requirements.
- Assess GI function for oral/enteral medications: nausea, vomiting, ileus, tube placement, and gastric motility all affect absorption.
- Assess skin integrity and perfusion at transdermal patch sites; impaired circulation reduces dermal absorption.
- Assess respiratory effort and presence of bronchospasm before administering inhaled medications.
- Assess concurrent medications and food intake that may alter gastric pH, GI motility, or compete with drug absorption.
- Assess life span factors that alter absorption (see Life Span Considerations).
Nursing Interventions
- Administer by the prescribed route; route changes alter pharmacokinetics and require a new prescriber order.
- Administer oral medications with or without food per drug-specific pharmacokinetic requirements.
- Verify formulation handling before administration: do not crush/chew enteric-coated or sustained-release forms unless product-specific guidance confirms safety.
- Rotate SC and IM injection sites to prevent tissue changes that impair local absorption.
- Never apply heat or cold over transdermal patches — altered skin blood flow significantly changes absorption rate and can cause toxicity (for example rapid fentanyl release).
- Assess and coach inhaler technique; poor technique reduces drug delivery to target airways.
- For IV administration, verify drug compatibility before co-infusing and maintain strict sterile technique.
Heat Over Transdermal Patches
Heat sources (heating pads, hot baths, electric blankets) applied over a transdermal patch dramatically increase skin vasodilation and drug absorption rate, which can rapidly cause life-threatening toxicity — particularly with fentanyl patches.
Life Span Considerations
Neonate and Pediatric
- Gastric acid-producing cells are immature until approximately age 1–2, altering gastric pH and affecting absorption of pH-sensitive oral drugs.
- Gastric emptying may be decreased due to slowed or irregular peristalsis, delaying drug transit and absorption.
- The immature liver has reduced first-pass elimination capacity, resulting in higher drug blood levels than adults receiving the same weight-adjusted oral dose.
Older Adult
- Decreased GI blood flow with aging reduces absorption efficiency of orally administered drugs.
- Changes in gastric pH can alter absorption of pH-sensitive medications.
- Reduced plasma protein availability increases the free (active) fraction of highly protein-bound drugs, elevating pharmacologic effect and toxicity risk.
- Decreased cardiac output reduces peripheral circulation and impairs SC and IM absorption in patients with circulatory compromise.
- Reduced subcutaneous fat decreases absorption from transdermal patches that require adequate subcutaneous tissue stores.
Pharmacology
| Route | First-Pass Effect | Bioavailability | Key Nursing Consideration |
|---|---|---|---|
| Oral / Enteral | Yes | Reduced | Gastric pH, motility, food, enteric coating affect absorption; multiple doses may be needed |
| IM / SC | No | High (variable) | Avoid with poor perfusion; rotate sites; can cause local tissue reactions |
| IV | No | 100% | Immediate onset; sterile technique required; verify drug compatibility before co-infusion; required dose may be lower than oral form because first-pass loss is avoided |
| Transdermal | No | Steady, slow | Small molecules only; avoid heat/cold over sites; assess subcutaneous tissue adequacy |
| Inhalation | No | Route-dependent | Particle size and patient technique determine pulmonary penetration depth |
Clinical Judgment Application
Clinical Scenario
An 82-year-old patient with heart failure is prescribed subcutaneous insulin. Despite consistent administration, postprandial blood glucose levels remain persistently elevated.
- Recognize Cues: Subtherapeutic glucose control in an older adult with heart failure receiving SC insulin at a consistent dose.
- Analyze Cues: Decreased cardiac output reduces peripheral tissue perfusion, impairing SC insulin absorption from injection sites.
- Prioritize Hypotheses: Impaired SC absorption secondary to reduced peripheral circulation is the most likely cause of subtherapeutic drug effect.
- Generate Solutions: Notify prescriber; assess injection sites; evaluate perfusion; consider site rotation or alternative insulin delivery strategies.
- Take Action: Document findings, assess all current injection sites for tissue changes or poor perfusion, and notify the prescriber for dose or route reassessment.
- Evaluate Outcomes: Blood glucose trends improve after prescriber-directed adjustment; patient educated on circulation-related absorption variability.
Related Concepts
- pharmacokinetics-and-pharmacodynamics — Absorption is the first of four ADME stages.
- distribution-pharmacokinetics — After absorption, drug distributes from systemic circulation to tissues.
- oral-medication-administration-safety — Procedure-level guidance for oral route including food/timing considerations.
- intravenous-medication-administration-safety — Procedure-level guidance for IV route with 100% bioavailability implications.
- medication-administration-safety-measures — System-level safeguards accounting for route-specific absorption risks.
Self-Check
- Which routes bypass the first-pass effect? Name at least three.
- Why might a neonate require a lower weight-based oral dose than an older child to achieve the same blood drug level?
- A patient with a fentanyl transdermal patch requests a heating pad for back pain. What is the nurse’s priority response and rationale?