Enteral Nutrition Support
Key Points
- Enteral nutrition is preferred when the GI tract is functional but oral intake is unsafe or insufficient.
- In palliative trajectories, enteral support may be considered when appetite remains but swallowing is impaired.
- Common routes include NG/OG (often short term, commonly under about 4 weeks) and PEG/PEJ (longer term).
- Safe care requires route verification, aspiration-prevention measures, and ongoing tolerance monitoring.
- The most serious feeding complication is respiratory aspiration of gastric contents, which can progress to life-threatening aspiration-pneumonia.
- Hydration safety requires reliable free-water administration when ordered; missed doses can cause dehydration and hypernatremia.
- During enteral medication passes, administer one medication at a time, flush before/between/after doses, and document flush totals in I&O.
- Before initiation, verify complete EN order components (formula, route, method, rate, and free-water flush plan) and reconcile concerns before feeding starts.
- In high-demand hypermetabolic states (for example severe burns), early enteral initiation (often within 24 hours when feasible) supports protein-calorie replacement.
Pathophysiology
Enteral feeding provides nutrients through the digestive tract, preserving gut integrity and physiologic nutrient handling. It is indicated when swallowing or oral intake is compromised but digestion/absorption remain adequate.
Classification
- Short-term access: NG or OG tube routes.
- Long-term access: PEG or PEJ routes.
- Additional route variation: Some organizations also use nasoduodenal (ND) routes in selected long-term or gastric-intolerance contexts per local policy.
- Delivery pattern: Continuous, intermittent, or bolus administration per care plan.
- Route-selection context: OG tubes are typically reserved for intubated/sedated clients; conscious clients generally require alternative access because gag/vomiting risk is higher.
- Common indication patterns: Coma or mechanical ventilation, high-demand catabolic illness (for example burns or critical illness), progressive neurocognitive/neuromuscular swallowing impairment (for example dementia or advanced Parkinson disease), severe anorexia during HIV/chemotherapy/sepsis care, and upper-GI obstruction/stricture/tumor.
- Post-stroke swallowing-risk pattern: Dysphagia is common after acute stroke; if oral intake is unsafe, early enteral planning (often within about 48-72 hours per team assessment) helps limit nutrition deficits during accelerated metabolic demand.
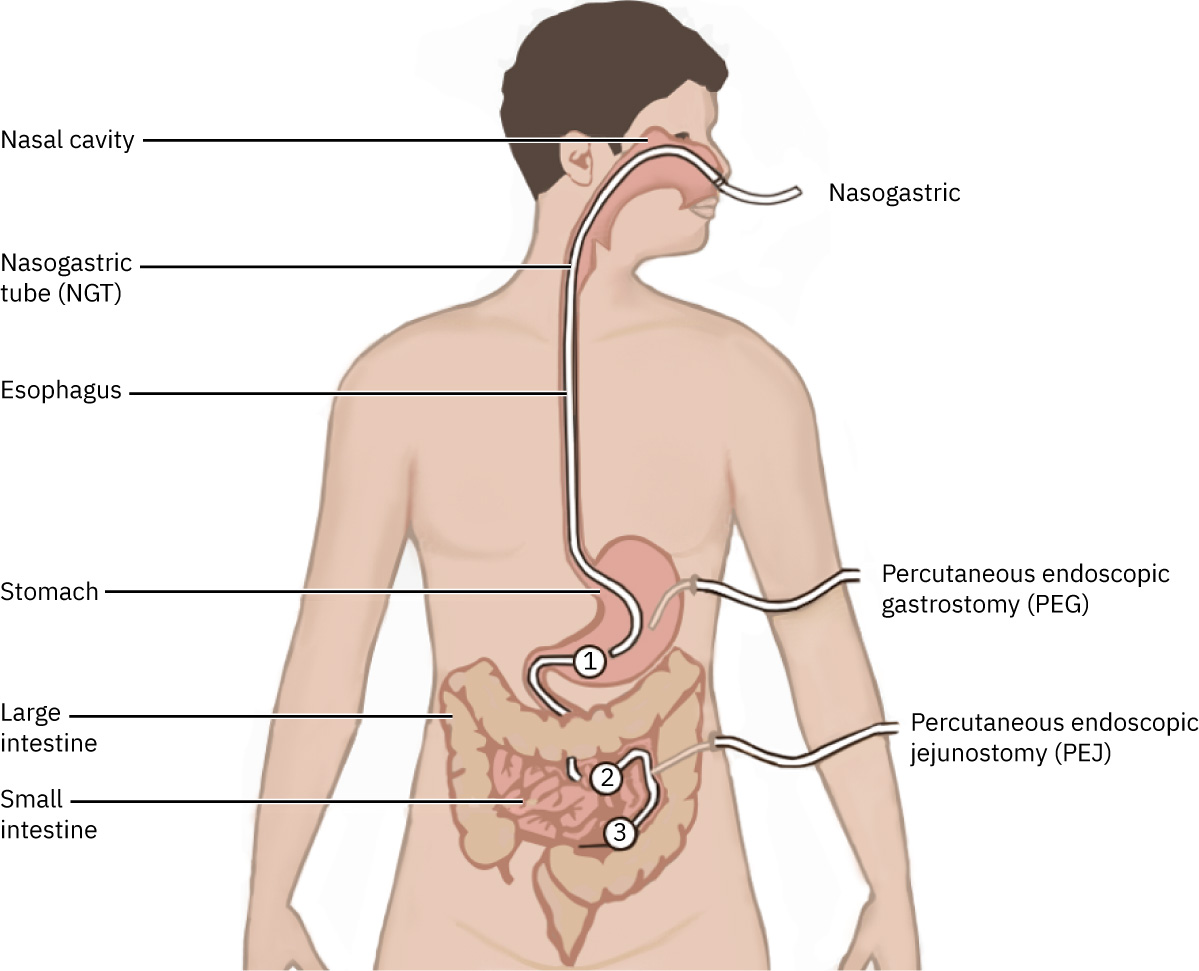 Illustration reference: OpenStax Clinical Nursing Skills Ch.17.3.
Illustration reference: OpenStax Clinical Nursing Skills Ch.17.3.
Nursing Assessment
- Assess feeding indication, GI function, aspiration risk, and current nutrition status.
- Assess tube position verification status and access-site integrity.
- Assess for leakage, insertion-site erythema/drainage, and skin-breakdown risk around enteral access points.
- Assess tolerance cues: abdominal distension, nausea/vomiting, cramping, diarrhea/constipation, and hydration pattern.
- Assess patient-reported psychosocial response to tube feeding, insertion-site discomfort, and cough/respiratory symptoms after feedings as potential intolerance or aspiration-warning cues.
Nursing Interventions
- Verify route and formula orders before each administration and recheck position before feed/med use per policy.
- Coordinate interdisciplinary planning with provider, dietitian, pharmacist, and bedside nursing team for formula choice, hydration plan, and administration method/rate.
- In acute stroke pathways with persistent dysphagia, avoid prolonged nutrition interruption; escalate early for alternate-route feeding once airway-swallow safety assessment is complete.
- For severe catabolic states (for example major burn or extensive wound healing), prioritize timely enteral-start workflows so protein-calorie goals are addressed early when oral intake is inadequate.
- Verify EN prescription completeness before initiation or major changes (formula type, route, administration method, infusion rate, and free-water flush amount/frequency).
- For NG/OG tubes, document external length after placement and trend migration each shift and with each use.
- Prefer evidence-based placement checks (visible external length versus X-ray-verified baseline, reassessed at scheduled intervals and before feed/med administration) instead of unreliable bedside methods such as auscultatory air-instillation tests.
- Use aspirate pH checks only as an adjunct when permitted by policy; if placement remains uncertain, hold use and obtain definitive verification.
- Follow tube-placement confirmation and flush protocols per policy, including flushes before/after intermittent feedings and medication administration.
- Reinforce routine tube flushing every shift and as needed to reduce occlusion risk.
- For enteral medication administration, prepare each medication separately, dilute per policy/order, and avoid mixing multiple medications in the same cup/syringe.
- If continuous/intermittent feeding is running, pause feedings based on medication requirements (for example incompatibility with feeding, empty-stomach requirement, or placement-check workflow) and resume per order/policy.
- If gastric feeding is poorly tolerated (for example delayed gastric emptying patterns), anticipate provider/dietitian reassessment for post-pyloric or jejunal enteral-delivery strategies.
- Administer ordered free-water volumes with medication-level reliability and document each dose per policy.
- Elevate head of bed to at least 30 degrees during enteral therapy (and after feeds as ordered) to reduce aspiration risk.
- Keep head of bed about 30-45 degrees as tolerated during feeding and after administration per plan.
- During enteral medication passes, keep head of bed at least 30-45 degrees and continue elevation for about 60 minutes after administration unless continuous feeding plan specifies otherwise.
- Monitor intake/output, electrolyte and glucose trends, weight trend, and complications; escalate promptly when abnormal.
- Evaluate gastric residual and feeding-intolerance context together; avoid unnecessary feeding interruption for lower residual volumes when no other intolerance signs are present and policy allows.
- For GRV workflows, avoid routine feeding interruption for residual volumes below about 500 mL when no other intolerance signs are present and policy allows.
- If residual assessment is performed per policy and tube placement is confirmed, follow policy-directed handling of aspirate (many workflows return residual into the gastric tube unless contraindicated).
- If bolus cramping occurs, consider room-temperature formula and reassess tolerance pattern.
- Follow flush protocols rigorously (for example before/after feedings and medication administration, plus scheduled patency flushes) and monitor tubing for migration/obstruction each shift and each use.
- If tube clogging occurs, use warm-water flushing with a 60-mL syringe as first-line declogging; avoid acidic flushes (for example cranberry juice or carbonated beverages) that can worsen occlusion.
- Use enteral-specific connection safety practices (for example EnFit-compatible pathways), avoid ad-hoc IV/feed adapters, and trace lines to origin during reconnection/handoff to reduce misconnection harm.
- Perform line reconnections under adequate lighting, verify all connections are secure, and label tubing at proximal/distal ends per policy to reduce misconnection errors.
- For medication passes, flush at the beginning, between medications, and at the end (adult practice commonly uses at least 15 mL water each flush unless fluid restriction/policy directs otherwise).
- If tube suction is active for decompression, disconnect suction during medication administration and commonly hold/clamp about 20-30 minutes before reconnecting to support medication absorption.
- For gravity/bolus feedings, maintain head-of-bed elevation at or above 30 degrees during infusion and for at least about 1 hour afterward unless contraindicated.
- Inspect insertion/exit sites for leakage, erythema, and purulent drainage; report abnormalities promptly.
- For PEG/PEJ external insertion sites, perform daily cleansing per policy (commonly gauze moistened with water or saline, then air dry before fixation-plate repositioning) and use barrier protection when skin breakdown risk is present.
- Document each feeding/irrigation session with amount delivered, irrigation solution and flush volume, residual findings (amount/color/odor/consistency when measured), placement-check method, and patient tolerance per policy.
- Escalate if scheduled free-water doses are missed or if concentrated formula plans lack hydration coverage, especially in clients unable to report thirst.