Ischemic Stroke Acute Treatment and Secondary Prevention
Key Points
- About 87 percent of strokes are ischemic and require rapid reperfusion-focused care.
- Immediate non-contrast head CT distinguishes ischemic from hemorrhagic stroke before thrombolytic use.
- Reperfusion options include IV thrombolytics (3 to 4.5 hour window) and mechanical thrombectomy (selected large-vessel cases up to 24 hours).
- Postacute care prioritizes recurrent-stroke prevention, neurologic complication monitoring, and rehabilitation planning.
- In acute workflows, recent anticoagulant exposure with elevated INR can contraindicate thrombolysis despite time-window eligibility.
Pathophysiology
Ischemic stroke occurs when cerebral perfusion is interrupted by intravascular occlusion rather than vessel rupture. Occlusions may form in cerebral vessels (thrombotic) or embolize from extracranial/cardiac sources.
Major ischemic categories include large-artery thrombosis, small-vessel (lacunar) thrombosis, cardiogenic embolism, and cryptogenic stroke. Cardioembolic sources commonly include atrial fibrillation, valvular disease, recent myocardial infarction, and selected structural defects such as patent foramen ovale.
Transient ischemic attack (TIA) causes stroke-like deficits that resolve without permanent infarction but remains a major warning event because short-term recurrent-stroke risk is high.
Clinical Pattern Cues
- Large-vessel ischemia: Often sudden severe deficits (motor, sensory, language, visual, balance).
- Lacunar/small-vessel ischemia: Frequently more focal unilateral deficits with smaller functional territory involvement.
- Common warning clusters: Facial droop, unilateral arm/leg weakness, dysarthria/aphasia, visual changes, ataxia, dizziness/vertigo.
Assessment and Diagnostics
NCLEX Focus
First identify last-known-well time and activate stroke pathway, then confirm stroke type and reperfusion eligibility.
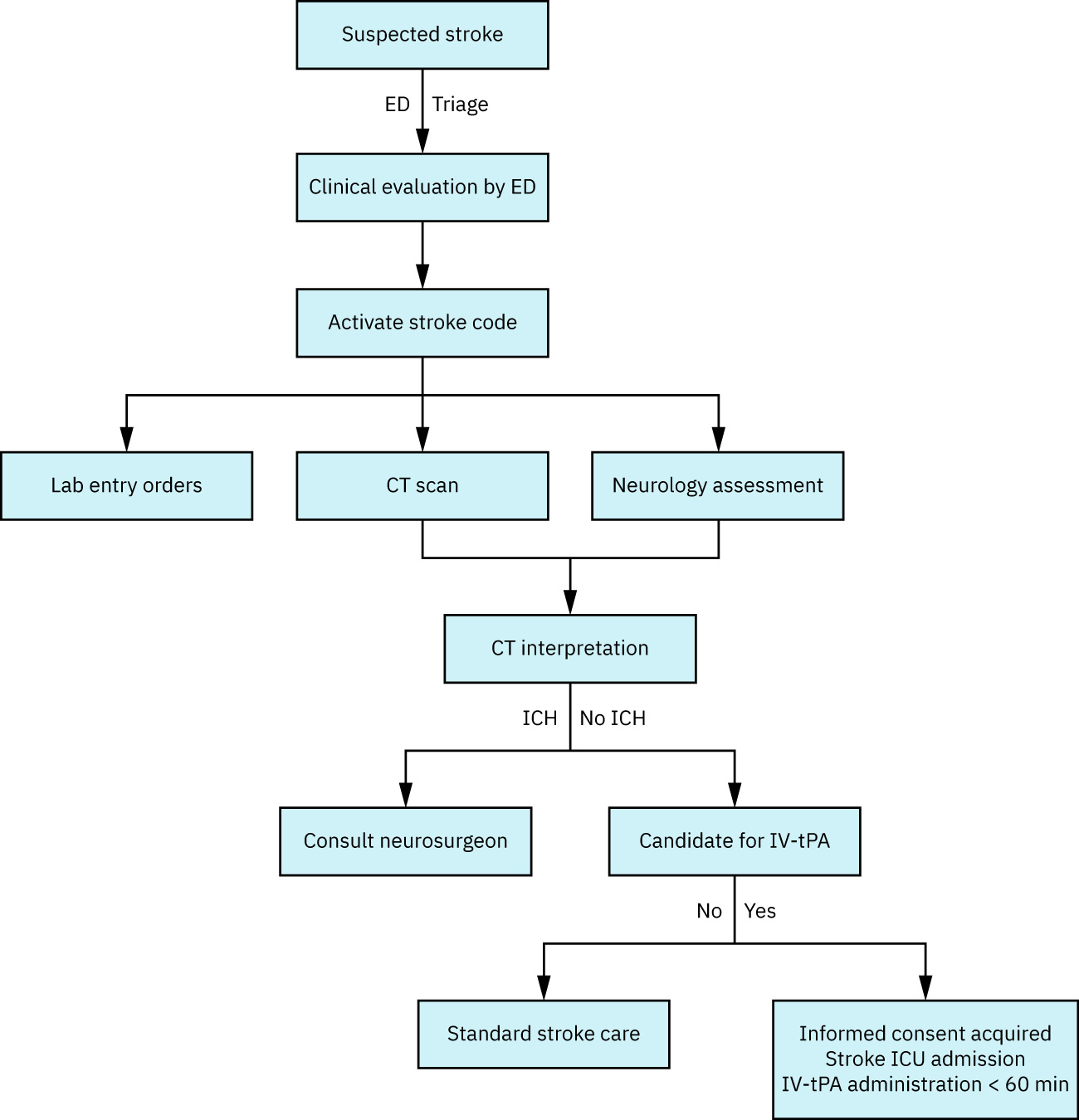 Illustration reference: OpenStax Fundamentals of Nursing Ch.8.1.
Illustration reference: OpenStax Fundamentals of Nursing Ch.8.1.
- Obtain last-known-well time immediately because treatment windows are time dependent.
- Perform focused neurologic exam with NIHSS scoring (higher score indicates greater severity and poorer prognosis trend).
- Collect focused risk history: hypertension, diabetes, prior stroke/TIA, smoking, hyperlipidemia, atrial fibrillation, oral contraceptive use, and cardiac disease history.
- Keep suspected stroke patients NPO until validated swallow screening is completed.
- Use structured early neuro-check cadence after activation (for example frequent q15-minute reassessment during initial high-risk period) per protocol.
Diagnostic Work-Up
- First-line imaging: STAT non-contrast head CT to exclude hemorrhage.
- Infarct characterization: MRI with diffusion-weighted imaging can define ischemic injury and penumbra.
- Vascular studies: CTA/MRA, angiography, or carotid ultrasonography to localize stenosis/occlusion.
- Cardioembolic evaluation: ECG/telemetry and transthoracic/transesophageal echocardiography.
- Laboratory studies: CBC/BMP, PT/INR/PTT/Xa context, glucose/A1C, lipid panel, ESR/CRP, D-dimer, and selected thyroid testing.
Nursing Interventions
- Activate emergency stroke response per facility protocol.
- Maintain airway and optimize cerebral perfusion (head/neck alignment, oxygen support per protocol, frequent vital/neurologic checks).
- Maintain NPO status until swallow safety is confirmed.
- Establish large-bore IV access and obtain accurate weight for weight-based thrombolytic dosing.
- Prepare for urgent imaging and time-critical reperfusion interventions.
- Monitor closely for deterioration and complications (new deficits, cerebral edema, seizure, hemorrhagic transformation).
Medical Therapies
Reperfusion
- IV thrombolysis: Alteplase or tenecteplase in eligible patients after hemorrhage exclusion.
- Thrombolytic window: Generally within 3 to 4.5 hours from last-known-well.
- Mechanical thrombectomy: Large-vessel occlusion pathway, selected patients up to 24 hours from onset.
Key Safety Considerations
- Screen contraindications before thrombolytics (for example significant coagulopathy, recent major bleeding/surgery, severe uncontrolled hypertension, active internal bleeding risk states).
- Include anticoagulation-context checks (for example elevated INR with current warfarin exposure) in thrombolytic contraindication screening.
- After thrombolysis, monitor closely for intracranial bleeding and repeat neuroimaging before starting antiplatelet/anticoagulant therapy per protocol.
- Blood-pressure targets are treatment-stage specific; permissive-hypertension strategy may be used initially to support penumbra perfusion.
Secondary Prevention
- Start antiplatelet strategy (aspirin-based, with selected dual-antiplatelet pathways by stroke severity/context).
- Use high-intensity statin therapy when indicated to reduce recurrent atherosclerotic risk.
- Optimize blood-pressure, glucose, lipid, and rhythm control.
- Coordinate early rehabilitation and social-work planning when deficits persist and discharge destination (home vs rehab) is uncertain.
- Reinforce risk-factor modification: smoking cessation, physical activity, weight management, healthy diet, and sleep-apnea management.
Clinical Judgment Application
Clinical Scenario
A hospitalized patient develops acute left facial droop, slurred speech, and left arm weakness during morning assessment.
- Recognize Cues: New focal neurologic deficits consistent with acute stroke warning signs.
- Analyze Cues: Findings suggest probable acute ischemic CVA requiring immediate type confirmation and reperfusion screening.
- Prioritize Hypotheses: Preserve viable brain tissue by minimizing door-to-imaging and door-to-treatment delays.
- Generate Solutions: Activate stroke team, maintain NPO, optimize oxygenation/perfusion, and expedite CT/NIHSS workflow.
- Take Action: Implement protocol-driven emergency interventions, obtain IV access/weight, and prepare for thrombolytic or thrombectomy pathway.
- Evaluate Outcomes: Reperfusion is initiated within target window, neurologic decline is limited, and prevention plan begins early.
Related Concepts
- stroke - Broad CVA framework including ischemic and hemorrhagic differentiation.
- hypertension-assessment-and-management - Major modifiable risk factor for first and recurrent stroke.
- anticoagulants - Cardioembolic prevention context and postacute treatment planning.
- dysphagia - Aspiration-risk screening and swallow-safety pathway in acute stroke care.
Self-Check
- Why is last-known-well time the first priority data point in suspected ischemic stroke?
- Which findings determine whether thrombolysis is safe and appropriate?
- How does permissive hypertension differ from routine chronic blood-pressure goals?