Stress Response Homeostasis and Allostasis
Key Points
- Stress is a physiologic response to a stressor that can be adaptive or harmful depending on duration and recovery.
- Homeostasis is baseline equilibrium; allostasis is the active physiologic adjustment process during challenge.
- Positive stress (eustress) can support healthy outcomes, while negative stress (distress) drives illness risk.
- Acute stress can support survival, while chronic unresolved stress drives maladaptive system changes.
- Stressors vary by origin and scale, including physiologic and psychosocial triggers ranging from major life events to daily irritations.
- Nursing care prioritizes symptom stabilization, stressor reduction, and support of effective recovery patterns.
Pathophysiology
Stress activation is a nonspecific biologic response: diverse stressors may produce similar core physiology despite different diagnoses. Threat appraisal pathways involving limbic-hypothalamic signaling engage hypothalamic-pituitary-adrenal and autonomic responses. A common sequence is hypothalamic CRH release, anterior-pituitary ACTH release, and adrenal corticosteroid output (especially cortisol), along with sympathetic activation.
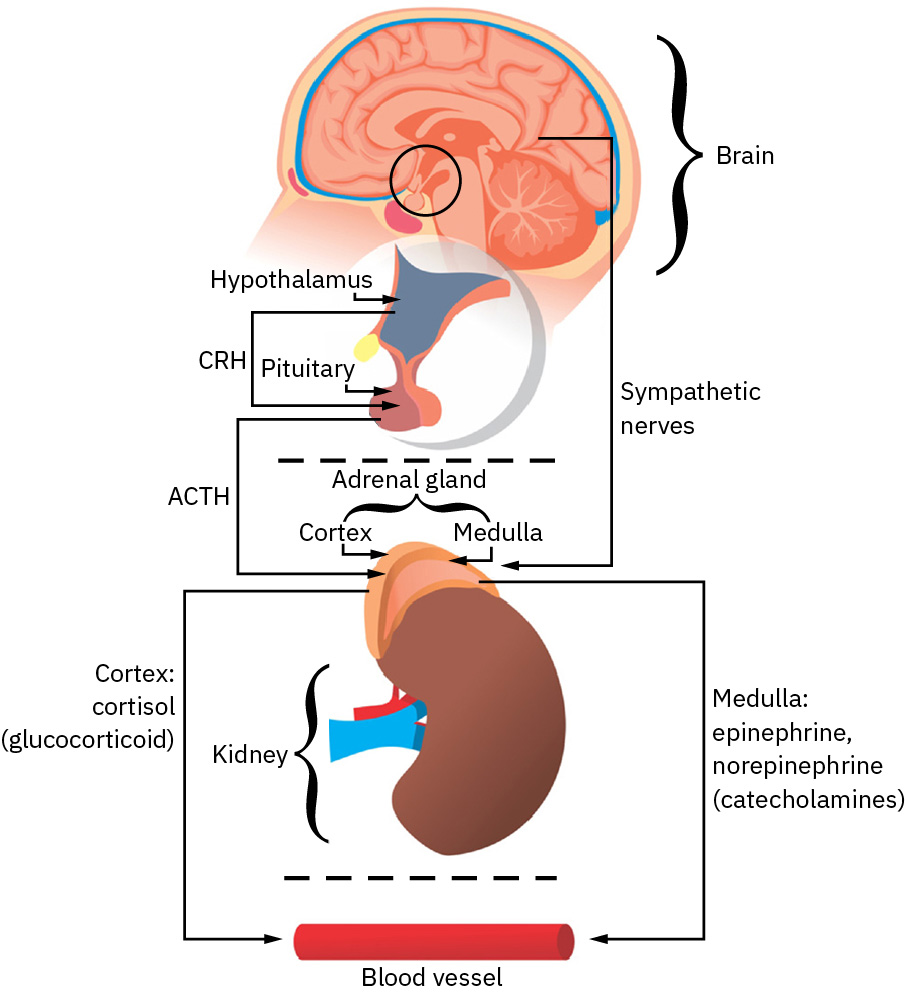 Illustration reference: OpenStax Fundamentals of Nursing Ch.34.1.
Illustration reference: OpenStax Fundamentals of Nursing Ch.34.1.
Cortisol and catecholamines (epinephrine, norepinephrine, and dopamine) support short-term survival responses such as increased heart rate, blood pressure, bronchodilation, and glycogen-to-glucose mobilization. At bedside, sympathetic-dominant adaptation commonly presents with muscle tension, pupillary dilation, and blood-flow redistribution away from digestion toward brain and skeletal muscle demand. With prolonged activation, these same mechanisms can contribute to constipation, chronic hyperglycemia, fatigue, and broader adaptation decline.
Adaptation is the process of adjusting to internal or external change over time, and homeostasis is the physiologic balance state that adaptation attempts to preserve. Both physiologic stressors (for example illness, injury, pain, malnutrition, and temperature extremes) and psychosocial stressors (for example grief, interpersonal conflict, addiction, and role strain) can trigger this same biologic stress system. The transactional stress perspective adds that response intensity is shaped by person-environment interaction, including personal, social, environmental, spiritual, cultural, educational, and emotional-intelligence factors.
Behaviorally, acute threat responses may present as fight, flight, freeze, or fawn patterns. These variants reflect the same stress biology but differ in outward coping behavior.
When stress resolves, parasympathetic recovery and hormonal downregulation help restore equilibrium. If stressors persist, sympathetic signaling remains prolonged, shifting from adaptive response to maladaptive strain. If the stress response fails to restore homeostasis, persistent autonomic and inflammatory activation can become disease-promoting rather than protective. This emergency-oriented physiologic pattern is useful for acute survival but biologically costly when sustained as a chronic baseline state. Long-term cortisol exposure can suppress lymphocyte effectiveness and increase infection vulnerability.
Allostasis describes this dynamic process of adjustment under challenge. Repeated activation without adequate recovery increases physiologic burden and contributes to long-term dysfunction. When challenge exceeds coping reserve, allostatic load can transition to allostatic overload, increasing risk of progression from prolonged resistance into exhaustion-level dysfunction. Clinically, homeostasis aligns with stable baseline status (vital signs, laboratory patterns, and mental-state stability), whereas allostasis reflects ongoing biologic variability as challenge intensity changes. A practical thermoregulation example is heat-triggered sweating versus cold-triggered shivering to return body temperature toward baseline.
Physiologic homeostasis is regulated by feedback loops. In hypotension, stress signaling can increase cortisol and catecholamine output to support vasoconstriction and cardiac output, while aldosterone-mediated sodium/water retention helps restore circulating volume. In hypertension, compensatory vasodilation and renal excretion pathways help move blood pressure back toward baseline.
Homeostasis also has a psychological dimension. Whether stress begins as a physical threat or a psychological threat, the downstream neuroendocrine cascade is similar; distress may therefore present with emotional symptoms first, somatic symptoms first, or both. A psychophysiological lens is useful because mental and physical stress responses can become self-reinforcing cycles rather than isolated events.
Classification
- Stress patterns: Eustress (positive adaptive challenge) and distress (negative burden).
- Exposure-duration patterns: Acute stress with rapid resolution versus chronic stress with sustained physiologic activation.
- Stressor-origin patterns: Physiologic, psychosocial, and mixed stressor burden.
- Response-role patterns: Stress as stimulus (trigger) and stress as response (physiologic/behavioral manifestations).
- Stressor-scale patterns: Significant life changes, catastrophic events, frequent annoyances, and omnipresent irritations.
- Transactional-determinant patterns: Personal, social, environmental, spiritual, cultural, educational, and emotional-intelligence modifiers of appraisal and coping.
- Survival-response patterns: Fight, flight, freeze, and fawn.
- Equilibrium states: Homeostasis (steady baseline) and allostasis (active adjustment).
- Allostatic burden states: Allostatic load (cumulative strain) and allostatic overload (demand beyond coping capacity).
- Homeostasis domains: Physiologic equilibrium and psychological equilibrium with bidirectional mind-body influence.
- Feedback-control patterns: Negative and positive feedback mechanisms that restore or amplify targeted physiologic processes.
- Response quality: Effective adaptation with recovery versus ineffective adaptation with persistent strain.
- Clinical expression: Autonomic hyperarousal, endocrine strain, and behavior/coping changes.
- Self-regulation dimensions: Physiologic regulation, emotional self-regulation, and behavioral self-regulation.
Nursing Assessment
NCLEX Focus
Assess both physiologic signs and coping quality to distinguish short-term adaptation from harmful persistence.
- Assess stressor type, duration, and perceived controllability.
- Assess stressor origin (physiologic versus psychosocial) and scale (major event versus recurring daily burden).
- Assess transactional modifiers (personal/social/environmental/spiritual/cultural context, educational level, and emotional-regulation capacity) that alter response intensity.
- Assess mind-body crossover signs, including psychological stress presenting as somatic symptoms (for example chest or GI discomfort) and physiologic stress presenting as anxiety or distress.
- Assess autonomic and endocrine-linked cues (tachycardia, tachypnea, hypertension, pupil dilation, diaphoresis, sleep disruption, hyperarousal symptoms).
- Assess for prolonged sympathetic-overdrive consequences (constipation, chronic hyperglycemia, persistent fatigue, and infection susceptibility).
- Assess sympathomimetic contributors (for example heavy caffeine intake, cocaine, or indicated adrenergic medications) when autonomic activation appears disproportionate.
- Assess whether current stress response is recovery-oriented or disease-promoting (persistent inflammatory/autonomic burden without return toward baseline).
- Assess recovery indicators, including ability to return to baseline after stress episodes.
- Assess coping methods and whether they are adaptive or maladaptive over time.
Nursing Interventions
- Use targeted symptom stabilization to reduce immediate physiologic risk.
- Match intervention to stressor origin: treat physiologic causes to restore equilibrium and pair psychosocial causes with coping/support interventions.
- Tailor interventions to transactional context so plans align with the patient’s social supports, culture/spiritual framework, and health-literacy level.
- Use integrated mind-body interventions when needed, combining behavioral/cognitive stress management with indicated physiologic therapies.
- Initiate rapid autonomic down-regulation techniques such as paced diaphragmatic breathing during acute stress response.
- Teach brief meditation/calm-breathing practice as a practical way to reduce heart rate and blood pressure through autonomic modulation.
- Coach individualized stress-management and coping practices that are realistic for the patient context.
- Support restoration behaviors (sleep, hydration, activity pacing, social support use).
- Teach emotional and behavioral self-regulation framing: feelings can be acknowledged while actions remain values-consistent.
- Reassess trend trajectories to confirm movement back toward homeostatic function.
Persistent Activation Risk
Unresolved stress activation can progress into chronic disease patterns and psychosocial decline.
Pharmacology
Medication may treat stress-related symptom clusters, but pharmacologic support should be paired with stressor reduction and coping interventions to prevent recurrent physiologic activation.
Clinical Judgment Application
Clinical Scenario
A patient reports months of work and caregiving strain with insomnia, palpitations, and elevated blood pressure.
- Recognize Cues: Prolonged stress exposure, autonomic symptoms, and poor recovery.
- Analyze Cues: Pattern suggests allostatic strain rather than brief adaptive stress.
- Prioritize Hypotheses: Prevent progression to chronic cardiometabolic and mental-health impact.
- Generate Solutions: Combine symptom care with coping-plan redesign and support activation.
- Take Action: Implement monitoring, education, and referral pathways.
- Evaluate Outcomes: Improved sleep, lower physiologic activation, and better daily function.
Related Concepts
- general-adaptation-syndrome-and-stress-phase-nursing-interpretation - Stage-based stress progression model.
- chronic-stress-allostatic-load-and-system-breakdown - Long-term physiologic consequences of unresolved stress.
- stress-crisis-staging-and-type-specific-nursing-response - Escalation recognition and intervention timing.
- stress-and-anxiety - Symptom overlap and psychosocial management.
- healthy-people-2030-health-equity-and-social-determinants - Lifestyle adaptation framework for recovery.
Self-Check
- How do homeostasis and allostasis differ in clinical interpretation?
- Which findings suggest transition from adaptive to maladaptive stress response?
- Why must recovery capacity be assessed in addition to stressor intensity?