Family Dynamics Stress ACEs and Multisystem Health Outcomes
Key Points
- Healthy family dynamics reduce stress load and support coping, sleep, and behavioral stability.
- Dysfunctional dynamics and adverse childhood experiences increase risk for mental illness, substance use, and chronic disease.
- Family communication quality shapes resilience, adherence, and recovery during acute and chronic illness.
- Early identification and family-level interventions can interrupt intergenerational risk cycles.
- ACE burden is dose-related: higher exposure is linked to more adolescent risk behaviors, higher adult chronic-disease burden, and shorter life expectancy.
- Most adults report at least one ACE, and four or more ACEs are associated with lower educational attainment and unemployment risk.
- U.S. adult ACE burden is high (about 61% with at least one ACE; 16% with four or more), with disproportionate four-or-more burden in females and many racial/ethnic minority populations.
- In a 2024 child-population meta-analysis, 15% had four or more ACEs, with heavier burden in residential-care, juvenile-offending, and Indigenous populations.
- Positive family dynamics improve sleep quality, stress regulation, and relationship resilience, especially in adolescents.
- Illness can destabilize family function (disequilibrium, conflict, role strain) but may also increase cohesion when coping systems are strong.
Pathophysiology
Family stress and relational instability activate chronic stress pathways, increasing allostatic burden and affecting neuroendocrine, cardiovascular, metabolic, and behavioral outcomes. Repeated adverse exposures in childhood can alter developmental trajectories and coping patterns.
Early biologic vulnerability may begin prenatally. Maternal anxiety/depression burden and disrupted early attachment can alter infant cortisol patterning, increasing later psychopathology risk when protective supports are limited.
Positive dynamics (secure attachment, constructive communication, consistent support) buffer stress physiology and improve long-term outcomes. Negative dynamics (violence, neglect, chaos, isolation) amplify risk and worsen disease management.
Classification
- Protective dynamics: Cohesion, emotional responsiveness, adaptive communication, shared healthy habits.
- Risk dynamics: Conflict escalation, communication breakdown, neglect/abuse, instability, substance misuse.
- ACEs domains: Violence exposure, parental mental illness/substance use, housing/food insecurity, loss/separation, and traumatic caregiver relationships that alter self-concept and future relationship patterns.
- Childhood stress-response continuum: Positive stress (brief mild activation), tolerable stress (larger but time-limited activation buffered by supportive adults), and toxic stress (frequent prolonged adversity without buffering support) with toxic stress driving neurodevelopmental and long-term disease risk.
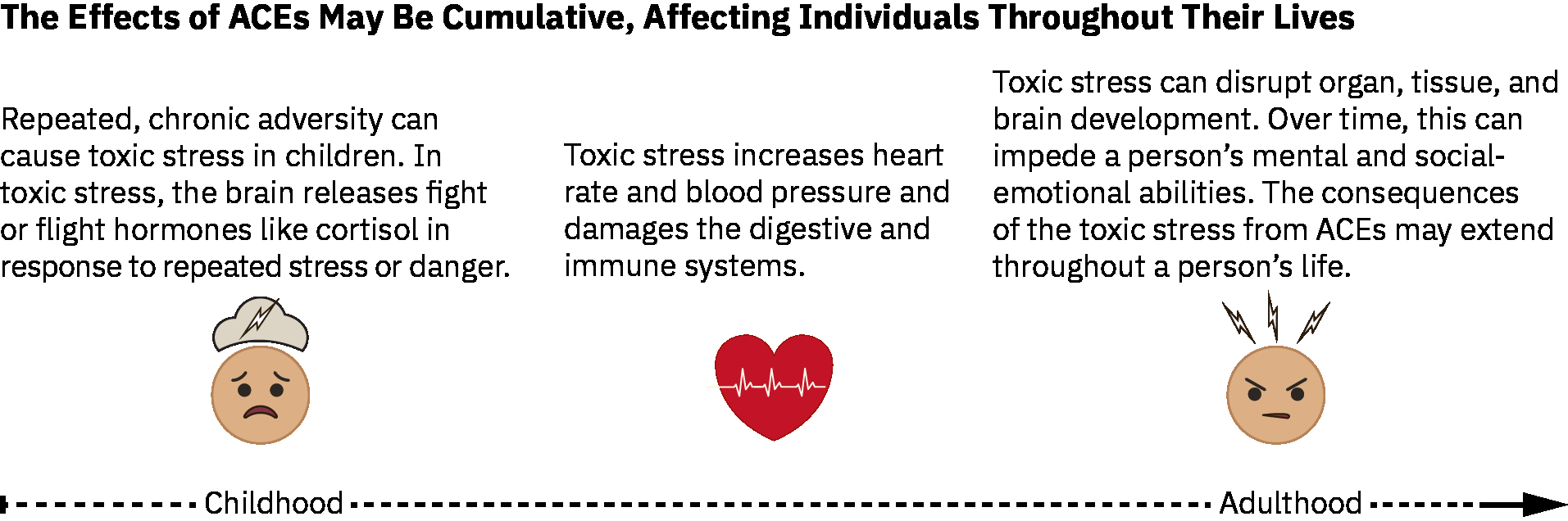 Illustration reference: OpenStax Population Health for Nurses Ch.27.6.
Illustration reference: OpenStax Population Health for Nurses Ch.27.6.
- Family risk-factor domains: Caregiver developmental/knowledge limitations, prior caregiver abuse history, financial strain, inconsistent discipline, low supervision, social isolation, and high interpersonal conflict.
- Family-system stressor framework: Demands, control, support, relationships, role clarity, and major change events.
- Community risk-factor domains: Violence/crime burden, poverty/unemployment, food insecurity, unstable housing, substance availability, and low youth/community engagement.
- Protective-factor domains: Stable nurturing relationships, basic-needs security, supportive mentor access, positive parenting, school engagement, and community childcare/after-school supports.
- Outcome domains: Anxiety/depression, addiction risk, sleep disturbance, cardiometabolic and functional decline.
- Extended ACE outcome domain: Higher ACE burden is linked to risky sexual behavior and increased long-term malignancy/cardiovascular/metabolic disease risk.
- Pediatric burden anchor: In one pediatric population comparison, children with 3 or more reported ACEs had markedly higher prevalence of mental/emotional/behavioral disorders versus those with 0 ACEs (36.3% vs 11.0%).
- Pediatric prevalence distribution anchor: In a 2024 meta-analysis across child populations, ACE prevalence was roughly 42% (0 ACE), 22% (1 ACE), 13% (2 ACEs), 8% (3 ACEs), and 15% (4 or more ACEs), with higher 4+ burden in residential-care, juvenile-offending, and Indigenous groups.
- Positive-outcome domains: Better sleep quality/duration, lower stress burden, stronger interpersonal conflict resolution, and improved illness recovery.
- Negative-disease-burden domains: Depression, anxiety, addiction, atherosclerotic/cardiometabolic risk, asthma/ulcer burden, and broader chronic-disease amplification under persistent dysfunctional dynamics.
- Coping-style domains: Meaning-focused, problem-focused, and emotion-regulation-focused patterns with mixed-strategy use as the common real-world pattern.
Nursing Assessment
NCLEX Focus
Assess family stressors as clinical risk factors, not background social details.
- Assess family communication patterns and coping style under stress.
- Assess current family stressor load using common triggers (for example housing change, role confusion, death/divorce, financial strain, overloaded schedules, serious illness, and work-life imbalance).
- Assess ACE-related exposures and current safety concerns.
- Assess health-behavior patterns (sleep, activity, diet, substance use) shaped by family context.
- Assess role strain and caregiver burden during illness-related role shifts.
- Assess child/adolescent risk behaviors and chronic-risk trajectory when ACE burden is high.
- Assess family and community protective assets that can be mobilized immediately (mentors, school supports, childcare, housing, and financial resources).
- Assess transition-phase stress in launching/senior life-cycle periods (for example empty-nest grief, role/livelihood changes, intergenerational dependence shifts).
- Assess for maladaptive coping cues (for example avoidance/isolation, relationship sabotage, substance misuse, or high-risk dopamine-seeking behaviors).
- Assess visible family-level stress reactions such as escalating arguments, withdrawal/disconnection, overuse of food/alcohol/substances, and failure to meet essential role duties.
- Assess illness-phase burden on family functioning, including likely role reversal, “sick role” consolidation, and resentment risk when role changes are not openly negotiated.
Nursing Interventions
- Use trauma-informed, nonjudgmental communication to surface hidden stressors.
- Implement family-level coaching for sleep hygiene, stress regulation, and conflict de-escalation.
- Connect families to counseling, social work, and community resources early.
- Support early caregiver-infant bonding and perinatal mental-health referral when prenatal or postnatal stress burden is high.
- Reinforce protective routines and strengths to build sustainable resilience.
- Teach coping-strategy selection explicitly (meaning-focused vs problem-focused vs emotion-focused) and normalize combination use over time.
- Support ACE prevention with parent education, consistent supervision/discipline coaching, and linkage to economic, housing, and mental-health resources.
- Use the CDC ACE-prevention framework when planning community actions: strengthen economic family supports, promote nonviolence social norms, ensure a strong start for children, teach coping/relationship skills, connect youth to caring adults and activities, and intervene early to reduce short- and long-term harm.
- Include population-prevention pathways when available: economic family supports, high-quality childcare/preschool, healthy-relationship education, and youth-to-caring-adult connection programs.
- Collaborate with community pathways (for example after-school programs and safe childcare/preschool supports) to reduce ongoing exposure risk.
- Normalize help-seeking for parenting stress, substance misuse, depression, and suicidal thoughts to reduce ACE-related stigma barriers.
- In routine encounters, identify ACE risk cues early and refer youth/families to evidence-based prevention and support services.
- During illness-triggered role shifts, facilitate structured role renegotiation to prevent unsafe burden concentration and unresolved resentment.
- Apply primary ACE prevention through upstream advocacy and linkage (for example affordable housing, living-wage/economic supports, food assistance, parenting support, and violence-prevention resources).
- Apply secondary prevention by identifying ACE exposure risk, assessing protective factors, and using standardized ACE-informed screening workflows only when referral/treatment pathways are available.
- Apply tertiary prevention by reducing downstream harm through trauma-focused counseling referral, social-support network building, and stress-regulation teaching (for example paced breathing and meditation).
Intergenerational Risk Reinforcement
Unaddressed ACE-related dynamics can perpetuate disease risk and dysfunction across generations.
Pharmacology
Medication plans are more effective when family stressors and adherence barriers are addressed alongside symptom treatment.
Clinical Judgment Application
Clinical Scenario
A family with repeated emergency visits shows poor sleep, high conflict, caregiver exhaustion, and adolescent substance use.
- Recognize Cues: Multi-domain stress pattern with probable ACE carryover.
- Analyze Cues: Family dynamics are driving recurrent health instability.
- Prioritize Hypotheses: Immediate priorities are safety, stabilization, and coping infrastructure.
- Generate Solutions: Deploy family-centered counseling/referral and behavior-reset plan.
- Take Action: Coordinate interprofessional support and monitor adherence/response.
- Evaluate Outcomes: Reduced crises, improved function, and healthier family routines.
Related Concepts
- stress-response-homeostasis-and-allostasis - Mechanistic stress model underlying family-dynamics effects.
- chronic-stress-allostatic-load-and-system-breakdown - Long-term disease burden from unresolved stress.
- family-structure-perceptions-and-health-implications - Structural context shaping dynamic patterns.
- trauma-informed-care - Core approach for ACE-related assessment and intervention.
- substance-use-disorders - Frequent downstream manifestation of maladaptive coping environments.
Self-Check
- Which family-dynamics cues should trigger early prevention-focused intervention?
- How do ACEs contribute to later cardiometabolic and mental-health risk?
- Why are family-level interventions often necessary for durable individual outcomes?