Obsessive-Compulsive and Related Disorders
Key Points
- OCD features intrusive obsessions and compulsions that temporarily reduce anxiety but reinforce long-term cycles.
- OCD symptoms are typically time-consuming (often >1 hour/day) and impair work, school, or relationships.
- Lifetime psychiatric comorbidity is common; anxiety comorbidity is prominent in children, while depressive comorbidity is prominent in adults.
- Related disorders include body dysmorphic disorder, hoarding disorder, trichotillomania, and excoriation disorder.
- Exposure and response prevention (ERP) is a primary evidence-based treatment for OCD.
- When direct exposure is initially intolerable, imaginal exposure can be used to build habituation and readiness for broader ERP work.
- Habit reversal training (HRT) can be an effective adjunct for body-focused repetitive behaviors and selected habit-like compulsive patterns.
- Nursing care focuses on symptom tracking, coping support, medication monitoring, and stigma reduction.
Pathophysiology
OCD-related disorders involve dysregulated threat/salience processing, compulsive habit loops, and anxiety reinforcement. Neurobiological factors (including serotonergic pathway involvement), trauma/stress load, and learned behaviors contribute to chronicity. Imaging studies describe frontal-cortex and subcortical-pattern differences in many clients with OCD, although exact symptom-causation pathways remain under investigation.
Temporary relief after rituals strengthens repetition and functional impairment.
Classification
- OCD core cycle: Obsession → anxiety/distress → compulsion → temporary relief → recurrence.
- Common obsession themes: Contamination fears, taboo/forbidden thoughts, aggressive self-or-other harm thoughts, and symmetry/order preoccupation.
- Common compulsion patterns: Excessive cleaning/handwashing, rigid ordering/arranging, repetitive checking, and counting rituals.
- Insight specifier: Some clients recognize obsessive beliefs as excessive (good insight), while others have poor insight or delusional conviction.
- Clinical-severity cues: Time burden often exceeds one hour/day, behavior is hard to control, and rituals relieve distress without producing pleasure.
- Tic-related specifier context: A subset of clients with OCD also show motor or vocal tic symptoms.
- Risk-factor domains: Family history (especially first-degree relatives with early-onset OCD), neurobiologic circuit differences, and adverse childhood experiences.
- Pediatric postinfectious pattern: Some children show abrupt OCD-symptom onset/worsening after streptococcal infection (PANDAS context), followed by gradual improvement.
- Related disorders: Body dysmorphic, hoarding, trichotillomania, and excoriation presentations.
- BDD profile: Persistent preoccupation with perceived appearance flaws with repetitive checking/camouflaging/reassurance-seeking and high shame-withdrawal burden.
- Hoarding profile: Persistent difficulty discarding items regardless value, excessive acquisition patterns, and clutter that compromises safety/function.
- BFRB profile: Trichotillomania and excoriation often show tension/urge before behavior and temporary relief after behavior, followed by distress and visible tissue injury.
- Treatment strata: ERP/CBT first-line, adjunctive medication, and selected advanced interventions.
- Behavioral-adjunct strata: Imaginal exposure for high-distress fear content and HRT adjuncts for repetitive habit-like behaviors.
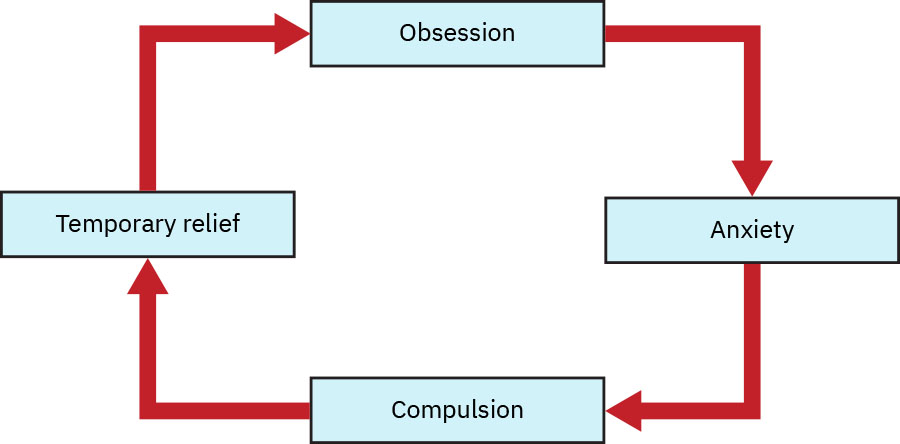 Illustration reference: OpenStax Psychiatric-Mental Health Nursing Ch.17.3.
Illustration reference: OpenStax Psychiatric-Mental Health Nursing Ch.17.3.
Nursing Assessment
NCLEX Focus
Assess time consumed by rituals and resulting functional impairment, not just symptom presence.
- Assess obsession themes, compulsion types, and daily time burden.
- Assess trigger patterns, avoidance, and distress severity.
- Assess skin/hair/body injury risks in body-focused repetitive behaviors.
- Assess whether contamination or checking compulsions are causing direct harm (for example dermatitis/skin breakdown, repetitive late departures, or safety-related functional disruption).
- In BDD patterns, assess time spent on mirror-checking/camouflage/reassurance seeking and evaluate social or occupational withdrawal linked to appearance preoccupation.
- In hoarding patterns, assess immediate home-safety hazards (fall/fire/respiratory risk), ADL obstruction, and family/caregiver burden.
- For hoarding severity trend, use structured tools when available (for example SI-R, HRS, CIR, and HEAL) alongside full clinical assessment.
- Assess comorbid depression, anxiety, and suicidality risk.
- Assess age-pattern comorbidity context (anxiety disorders commonly co-occur in children; depressive disorders commonly co-occur in adults).
- Assess readiness for ERP and family/support involvement.
- Assess whether rituals provide pleasure versus temporary anxiety relief; in OCD, compulsions generally relieve distress rather than produce pleasure.
- In children/adolescents, assess for less obvious rituals (for example blinking/breathing rituals), catastrophic family-harm fears, setting-specific symptom variability, and concealed symptoms.
- In children, assess insight limits and gather collateral observations from parents/teachers when obsessive-compulsive patterns are suspected.
- Assess trauma history, including adverse childhood experiences (ACEs), because childhood trauma is associated with obsessive-compulsive symptom burden.
- In children with abrupt OCD-symptom onset after recent streptococcal infection, escalate for medical evaluation of possible postinfectious neuropsychiatric patterns.
Nursing Interventions
- Support ERP principles and reinforce response-prevention adherence.
- Use imaginal exposure when in-vivo exposure is too overwhelming at treatment start, then transition toward broader ERP goals as tolerance improves.
- Teach distress-tolerance and anxiety-regulation strategies.
- Provide nonjudgmental education on disorder mechanisms and recovery trajectory.
- For BDD-focused care, use therapeutic communication that validates distress without reinforcing distorted appearance beliefs.
- Monitor medication effects and side effects for OCD-targeted regimens.
- Coordinate multidisciplinary supports for home safety and functional restoration.
- In hoarding care, coordinate family-inclusive planning, decluttering support, and environmental risk reduction in a collaborative nonshaming manner.
- Teach that OCD treatment response can be gradual; SSRI benefit may require 8-12 weeks and sometimes higher therapeutic dosing under prescriber supervision.
- If SSRI response is insufficient, support safe coordination of augmentation plans (for example antipsychotic add-on or advanced interventions such as TMS when indicated).
- Reinforce substance-risk counseling because some clients attempt to blunt obsessional distress with alcohol or drugs.
- Reinforce stress-management and routine-stabilization habits (consistent sleep schedule, regular exercise, balanced nutrition, and reliable support-person engagement).
- For habit-like compulsions and BFRBs, support HRT elements: awareness training, competing response practice, social reinforcement, motivation enhancement, and generalization across settings.
Ritual Accommodation Trap
Staff/family accommodation of compulsions may reduce short-term conflict but worsens long-term disorder severity.
Pharmacology
SSRIs are common first-line medications for OCD-related symptoms; dosing requirements are often higher than major-depression regimens and clinical benefit may require about 8 to 12 weeks. Clomipramine is a non-first-line option when SSRI response is inadequate or SSRI tolerability is poor. Short-term benzodiazepine use may be considered for acute anxiety burden but does not treat core OCD cycles and requires dependence-risk precautions. If SSRI response is insufficient, selected clients may benefit from antipsychotic augmentation, including clients with tic comorbidity.
For treatment-resistant adult OCD, repetitive transcranial magnetic stimulation (rTMS) may be used as an adjunctive option. Nursing education should include that sessions are typically outpatient and do not require anesthesia, with possible transient headache/light-headedness/jaw-facial tingling and rare seizure risk. Deep brain stimulation and gamma-knife procedures are reserved for severe refractory cases because of invasiveness/risk profile and are not first-line care.
Clinical Judgment Application
Clinical Scenario
A client spends hours daily washing, avoids touching household items, and develops skin breakdown while reporting “I know this is irrational but I cannot stop.”
- Recognize Cues: Classic obsession-compulsion cycle with physical harm and functional loss.
- Analyze Cues: Insight present, but anxiety reinforcement maintains compulsive behavior.
- Prioritize Hypotheses: Priority is safety plus ERP-oriented intervention.
- Generate Solutions: Build graded exposure plan, response prevention supports, and skin-care management.
- Take Action: Implement coordinated therapy/medication plan with daily monitoring.
- Evaluate Outcomes: Track ritual duration, distress tolerance, and functional recovery.
Related Concepts
- anxiety-related-disorders - Differentiates generalized/panic/phobic anxiety from OCD cycles.
- trauma-induced-and-stress-related-disorders - Addresses overlap with trauma-driven symptoms.
- self-harm-and-suicide - Guides risk planning in severe distress and comorbid depression.
- stress-and-anxiety - Provides foundational autonomic and coping context.
- client-engagement - Supports sustained participation in challenging ERP-based treatment.