Factors Affecting Self-Concept Across Health and Culture
Key Points
- Self-concept is continuously shaped by psychological, physiological, cultural, and behavioral influences.
- Stress, grief, anxiety, and depression can distort self-evaluation and reduce perceived competence.
- Illness, disability, pain, and aging-related changes can threaten identity, body image, and role confidence.
- Cultural norms, discrimination, social comparison, and media exposure can either strengthen or destabilize self-concept.
- Cultural body ideals vary widely; discordance between personal and social ideals can intensify body dissatisfaction and mental-health risk.
- Body-image stressors differ by life stage, including peer/media pressure in youth and relationship/work-role pressures in adulthood.
- Shame and rejection sensitivity can reinforce approval-seeking conformity and weaken authentic self-expression.
- Repeated success experiences can strengthen self-efficacy and self-esteem, while repeated failure can intensify inadequacy beliefs.
- Personality patterns, including Big Five trait tendencies, can modify how stressors are interpreted and integrated into self-concept.
- Stress subtype and duration matter: acute/eustress may be adaptive, while chronic distress is more likely to erode self-concept.
- Cultural adaptation pressure and gender-role expectations can reshape identity narratives and help-seeking behavior.
Pathophysiology
Self-concept reflects ongoing integration of internal states and external feedback. Persistent stress physiology and negative cognitive-emotional loops reduce psychological flexibility and magnify self-critical appraisal.
Health disruptions alter autonomy, appearance, and expected roles, which can trigger identity-threat responses. Without adaptive coping or social support, this often progresses to withdrawal, helplessness, and deteriorating self-worth.
Cultural context influences which traits are valued, how bodies are judged, and how success is defined. Misalignment between personal identity and social expectation can create chronic self-discrepancy and emotional distress.
When fear of rejection is high, individuals may prioritize external approval over authentic preferences. This shame-driven pattern can temporarily improve social acceptance while worsening long-term self-worth and emotional stability.
Body-image norms are not universal. Some settings emphasize thinness, while others value fuller body types; nurses should avoid assuming one standard and instead assess each patient’s cultural frame and lived meaning.
Social comparison patterns further shape self-concept. Upward comparison can motivate behavior change but may also worsen discouragement and nonadherence when patients view goals as unattainable; downward comparison may protect short-term morale but can mask unresolved risk behaviors.
Mastery history also matters. Accumulated success feedback often improves self-efficacy and positive self-appraisal, whereas repeated failure without supportive reframing can reinforce low-confidence identity narratives.
Stress effects are heterogeneous. Short-term stress or moderated eustress can support focus and growth, but persistent distress is more likely to produce anxiety, depressive symptoms, sleep disruption, and negative self-evaluation patterns that degrade self-concept.
Cultural and behavioral influences include social media comparison pressure, acculturation demands, and gendered role expectations. These forces can either strengthen belonging and purpose or increase stigma, suppression, and identity conflict.
Classification
- Psychological factors: Stress, grief, trauma, anxiety, depression, self-efficacy beliefs.
- Stress-pattern factors: Acute, episodic acute, chronic, eustress, and distress trajectories.
- Trait-profile modifiers: Big Five tendencies (openness, conscientiousness, extraversion, agreeableness, neuroticism) shaping appraisal style and coping expression.
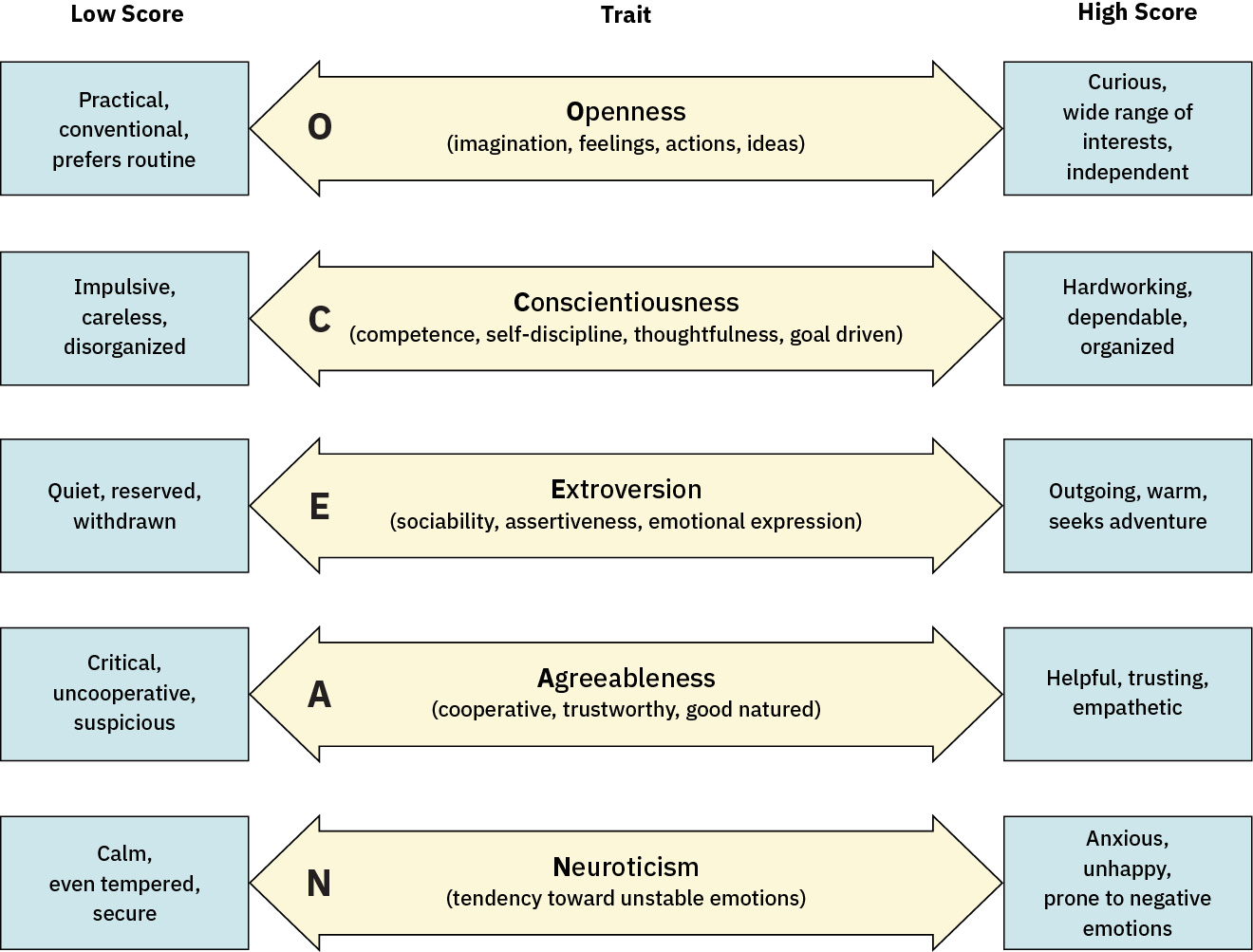 Illustration reference: OpenStax Fundamentals of Nursing Ch.32.2.
Illustration reference: OpenStax Fundamentals of Nursing Ch.32.2.
- Physiological factors: Aging, illness burden, disability, pain, sleep disruption, hormonal/neurochemical effects.
- Cultural factors: Identity norms, beauty standards, discrimination, acculturation stress.
- Gender-role expectation factors: Internalized masculinity/femininity norms influencing emotion expression, role identity, and support seeking.
- Body-image sociocultural drivers: Culture-specific ideals for body size, shape, and appearance attributes.
- Behavioral factors: Coping style, social interaction patterns, health behaviors, self-presentation patterns, and media-engagement habits.
- Comparison patterns: Upward versus downward social comparison and their impact on self-evaluation.
- Mastery-history factors: Prior success/failure and reinforcement quality across school, relationships, and work roles.
Nursing Assessment
NCLEX Focus
Identify both risk factors and protective factors; resilience assets change care planning decisions.
- Assess major life stressors, grief events, and perceived losses linked to identity change.
- Assess stress subtype and persistence (acute, episodic acute, chronic, and distress-heavy patterns).
- Assess illness- or disability-related threats to autonomy, role performance, and body image.
- Assess cultural context, stigma exposure, and belonging/safety within social environments.
- Assess social-media comparison burden and whether online feedback loops are worsening self-worth.
- Assess acculturation strain, discrimination exposure, and identity conflict across multiple cultural contexts.
- Assess body dissatisfaction severity and associated depression, anxiety, suicidal ideation, or obsessive appearance preoccupation.
- Assess life-stage drivers of body-image distress, including bullying, family/peer pressure, social-media comparison, relationship strain, and work-role expectations.
- Assess whether approval-seeking and conformity pressures are displacing authentic identity expression.
- Assess whether social comparison is improving motivation or worsening hopelessness, withdrawal, and treatment adherence.
- Assess prior success/failure narratives and current self-efficacy beliefs (“I can handle this” versus “I always fail”).
- Assess personality-linked response style, including perfectionistic conscientiousness, social inhibition, or high emotional reactivity.
- Assess gender-role pressure effects on emotional disclosure, coping, and willingness to seek help.
- Assess coping style quality (problem-solving versus avoidance) and self-care behavior patterns.
Nursing Interventions
- Normalize emotional responses to transition while reinforcing adaptive coping and self-efficacy.
- Collaboratively reframe health goals to preserve meaning, autonomy, and role participation.
- Teach stress-pattern recognition and intervention matching (for example acute grounding versus chronic-load recovery planning).
- Provide culturally responsive education and reduce stigma through respectful, individualized communication.
- Link patients to interdisciplinary supports for mental health, rehabilitation, and community connection.
- Initiate targeted referral when body-image distress is accompanied by eating-disorder risk behaviors or body dysmorphic features.
- Teach social-comparison harm reduction (media-literacy framing, realistic standards, and body-function focus) as part of routine support.
- Use shame-sensitive communication that separates human worth from performance, appearance, and social approval.
- Reframe progress using patient-specific baselines and functional goals rather than peer benchmarking.
- Build mastery-oriented goals that create frequent achievable successes to restore self-efficacy after repeated setbacks.
- Challenge rigid gendered coping expectations and normalize help-seeking as a strength behavior.
Isolation Spiral
Untreated self-concept erosion can lead to social withdrawal, nonadherence, and worsening mental-health risk.
Pharmacology
Medication effects on mood, cognition, appetite, sleep, and body composition can significantly influence self-concept and should be discussed transparently during care planning.
Clinical Judgment Application
Clinical Scenario
A recently diagnosed patient reports, “I am not the person I used to be,” avoids friends, and skips follow-up visits.
- Recognize Cues: Identity-loss language, social withdrawal, and adherence decline.
- Analyze Cues: Combined physiologic and psychosocial factors are destabilizing self-concept.
- Prioritize Hypotheses: Immediate focus is preventing isolation-driven deterioration.
- Generate Solutions: Build culturally relevant coping plan and role-restoration goals.
- Take Action: Initiate supportive counseling referral and structured follow-up.
- Evaluate Outcomes: Improved engagement, coping efficacy, and self-definition stability.
Related Concepts
- self-concept-components-and-lifespan-development - Foundational model for component-level interpretation.
- self-concept-measurement-and-clinical-assessment-tools - Methods to track factor-driven changes.
- nursing-support-for-self-concept-role-transition-and-coping - Intervention bundle for high-risk transitions.
- culturally-competent-care - Essential for context-sensitive psychosocial assessment.
- grief-and-loss - Common pathway for self-concept disruption after major life change.
- eating-disorder-risk-factors - Escalation pathway for body-image driven risk behaviors.
- obsessive-compulsive-and-related-disorders - Differential context for body-dysmorphic symptom patterns.
Self-Check
- Which factor clusters most strongly predict self-concept decline during illness?
- How can cultural norms become either protective or harmful to self-concept?
- Why should coping style be assessed alongside symptom burden?