Grief and Loss
Key Points
- Grief is a personal emotional response to meaningful loss and does not follow a fixed timeline.
- Mourning is the outward social expression of loss and is shaped by culture, rituals, personality, and prior life experience.
- Loss includes primary and secondary changes, such as shifts in identity, security, and future plans.
- Grief can include temporary identity confusion and existential questioning, especially after central role or relationship loss.
- Normal grief often includes mixed physical, emotional, cognitive, and behavioral reactions that fluctuate by person and context.
- Social support quality strongly influences grief adaptation and recovery.
- Nurses assess grief impacts on clients, families, and clinicians, including burnout and compassion fatigue risk.
- Grief evaluation starts at serious-illness diagnosis and continues through bereavement, with early escalation for safety-risk patterns.
Pathophysiology
Grief affects interconnected emotional, cognitive, physical, social, and spiritual systems. Persistent severe grief can increase risk for depression, anxiety, sleep problems, cardiovascular strain, and functional decline.
Protective adaptation is supported by validation, social connection, meaning-making, and individualized coping pathways. Acute grief physiology can include stress-hormone-driven vascular constriction, heart-rate and blood-pressure increase, and proinflammatory/coagulation shifts that intensify cardiopulmonary symptom burden in vulnerable adults.
Classification
- Grief patterns: Anticipatory, acute, integrated, and complicated/prolonged grief responses.
- NANDA framing:
GrievingandComplicated Grievingare core nursing diagnoses; legacy references may useMaladaptive Grieving. - Framework: Kubler-Ross stages (denial, anger, bargaining, depression, acceptance) as non-linear reference points that may repeat, overlap, or be skipped.
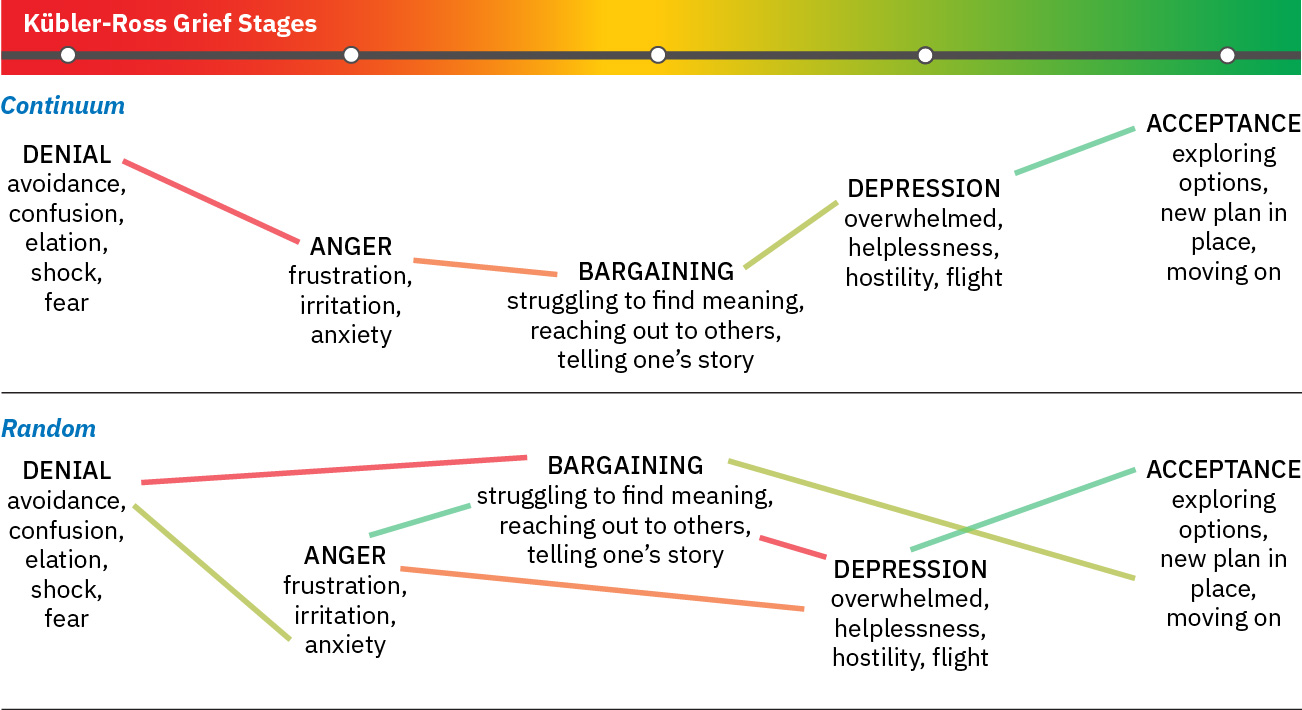 Illustration reference: OpenStax Fundamentals of Nursing Ch.36.1.
Illustration reference: OpenStax Fundamentals of Nursing Ch.36.1.
- Engel framework: Shock/disbelief, developing awareness, restitution, resolving loss, idealization, and outcome (commonly taught as a sequential heuristic).
- Bereavement period: Time after death when inner grief and outward mourning are processed and adaptation develops.
- Task framework: Notification/shock, experiencing the loss, and reintegration into life without the deceased.
- Mourning expression: Outward grief expression varies across cultural norms and family traditions.
- Term distinction: Grief is the internal response to loss, mourning is the outward expression, and bereavement describes the adjustment period after death.
- Disenfranchised-grief domain: Some losses receive limited social acknowledgment (for example miscarriage, nonrecognized relationships, or pet loss), increasing isolation risk.
- Impact domains: Physical, mental, social, spiritual, and occupational (including nurse burden).
- Identity-impact domains: Identity confusion, role reconstruction, and meaning-making after major loss.
- Normal-grief symptom domains:
- physical examples: chest tightness, palpitations, breathlessness, fatigue, dry mouth
- emotional examples: numbness, sadness, fear, anger, guilt, loneliness, yearning
- cognitive examples: confusion, poor concentration, depersonalization, dreams/sense of presence
- behavioral examples: crying, withdrawal, overreactivity, work-performance decline, reminder avoidance
- DSM-5-TR prolonged grief disorder context: Persistent intense longing/preoccupation beyond 12 months with functional impairment, plus at least 3 features such as disbelief, avoidance, identity disruption, emotional pain, reintegration difficulty, numbness, meaninglessness, or intense loneliness.
Nursing Assessment
NCLEX Focus
Distinguish normal variation in grief from complicated grief requiring escalated support.
- Assess type of loss and secondary-loss burden (role, identity, routine, security).
- Begin grief assessment at diagnosis/admission for acute, chronic, or terminal illness and continue through the survivor bereavement period.
- Assess anticipatory-loss themes (loss of independence, role, function, or expected milestones) before death occurs.
- Assess identity confusion cues (“part of me is gone”) and existential distress after major relational or role loss.
- Assess current grief expression, coping style, and support-system adequacy.
- Assess common normal-grief symptom clusters across physical, emotional, cognitive, and behavioral domains.
- Assess for cardiopulmonary alarm overlap (for example chest pain, dyspnea, palpitations, new murmur, rhythm change) because severe acute grief can mimic acute coronary presentations.
- In older adults after sudden loss, consider stress-induced cardiomyopathy risk and escalate urgent cardiac evaluation when symptoms suggest ACS.
- Differentiate grief from major depression: grief is often wave-like with preserved self-esteem, while major depression is more persistently low with worthlessness/self-loathing features.
- Screen for maladaptive depressive-coping patterns, including alcohol/drug self-medication and severe functional withdrawal.
- Assess withdrawal/isolation severity and risk for depression or safety concerns.
- Assess pressure from social “grieving rules” (for example expectations to recover quickly or grieve in a specific style) that may suppress healthy expression.
- During early bereavement, monitor for high physiologic stress burden and counsel survivors to defer major irreversible life decisions when feasible.
- Assess family powerlessness/guilt and perceived inability to help during active dying.
- Assess caregiver knowledge gaps about diagnosis trajectory, likely crisis patterns, and immediate post-death steps in home settings.
- Screen for complicated-grief risk factors (for example traumatic or sudden death, child loss, multiple recent losses, unresolved prior grief, low social support, and loneliness).
- In children/adolescents, assess developmental grief expression (for example regression or incontinence in younger children, versus social withdrawal, school decline, substance experimentation, or suicidality in older youth).
- In infants/toddlers, assess separation-distress patterns (irritability, sleep/eating disruption, caregiver-emotion reactivity) rather than verbal grief narratives.
- In preschool and early-childhood groups, assess magical-thinking self-blame (“I caused this”), death-reversibility beliefs, and play-based grief expression.
- In middle-childhood and preadolescent groups, assess emerging death-finality understanding with alternating emotional suppression, outbursts, and role imitation of the deceased.
- Recognize high-intensity survivor contexts (spousal loss and parent/grandparent child-loss grief) and prioritize early bereavement support.
- Assess spiritual distress versus resilience resources and meaning frameworks.
- Assess nurse emotional load and signs of compassion fatigue in high-loss settings.
- Escalate promptly for endangerment cues such as suicidal ideation, severe depressive progression, or prolonged high-intensity symptoms beyond expected adaptation windows.
Nursing Interventions
- Provide empathetic listening and normalize non-linear grief trajectories.
- Avoid rigid expectations about timing or “right” expression of grief.
- Validate disenfranchised losses explicitly and provide the same therapeutic support standards used for socially recognized bereavement.
- During anger-phase responses, provide a safe space for emotional ventilation while maintaining respectful communication boundaries.
- Use supportive presence and guided reminiscence to help families express meaning and connection during active dying and early bereavement.
- Connect clients/families to grief counseling, group support, and community resources.
- Use structured coping-enhancement steps: define short- and long-term goals, identify available resources, split complex tasks into manageable steps, and reinforce realistic hope.
- Reinforce that grief-stage reactions can occur with non-death losses (for example divorce, job loss, or major chronic-disease diagnosis), and tailor support accordingly.
- In high-stress periods, use calm reassurance, support limited realistic choices, and defer major irreversible decisions when possible.
- Encourage bereaved individuals to talk about the death and normalize expression of grief over time.
- Facilitate grief work by exploring initial reaction, memories, fears, prior loss experiences, and culturally meaningful mourning practices.
- Connect families to bereavement follow-up resources, including hospice programs, memorial services, support groups, and counseling/psychotherapy.
- Involve families in feasible bedside-care tasks to reduce helplessness and strengthen connectedness with the patient.
- Provide anticipatory teaching on expected dying changes and immediate after-death workflow to reduce panic and confusion.
- In pediatric grief support, use direct language such as “death” (avoid confusing euphemisms like “gone to sleep”), use play therapeutically, and involve grief specialists when risk cues are present.
- Use grief-supportive communication: prioritize listening/presence, avoid minimizing or presumptive phrases, and validate the person-specific grief experience.
- Integrate spiritual care supports when requested by client/family.
- Use team debriefing, reflective practice, and self-care planning for nurses.
Timeline Pressure Harm
Pressuring clients to “move on” can worsen shame, isolation, and prolonged grief symptoms.
Pharmacology
Pharmacologic care may address associated symptoms (for example, severe insomnia, anxiety, or depressive syndromes). Antianxiety medications or antidepressants may be prescribed when clinically indicated, but plans should remain grief-informed and paired with psychosocial interventions.
Clinical Judgment Application
Clinical Scenario
A recently bereaved client reports severe sleep disruption, social withdrawal, guilt, and inability to perform daily responsibilities for several months.
- Recognize Cues: Functional impairment and prolonged severe symptoms suggest complicated grief risk.
- Analyze Cues: Current coping and support structures are insufficient.
- Prioritize Hypotheses: Priority is safety, stabilization, and structured grief-focused support.
- Generate Solutions: Initiate referral to specialized grief therapy and strengthen support network.
- Take Action: Implement monitoring plan, education, and coordinated multidisciplinary follow-up.
- Evaluate Outcomes: Track function, sleep, social engagement, and distress intensity over time.
Related Concepts
- death-and-dying - Provides context for anticipatory and post-death adjustment needs.
- continued-support - Extends grief care through post-discharge and community follow-up.
- peer-support - Enhances connection and reduces isolation during bereavement.
- trauma-informed-care - Supports clients with traumatic grief features.
- mental-health-recovery-and-wellness - Guides long-term adaptation and resilience building.