Acne Vulgaris
Key Points
- Acne is a common skin disorder, especially in adolescence, but can occur across the lifespan.
- Core lesions include comedones, papules, pustules, nodules, and cysts.
- Disease activity is driven by androgen-sebum effects, follicular keratin changes, and inflammatory bacterial pathways.
- Most treatment is outpatient and combines topical therapy, selected oral agents, and adherence-focused education.
- Nursing priorities include trigger review, medication-safety monitoring, and scar-risk reduction.
Pathophysiology
Acne develops in pilosebaceous units through interacting mechanisms: increased androgen influence, increased sebum production, altered follicular keratinization, and inflammatory response linked to Cutibacterium acnes colonization.
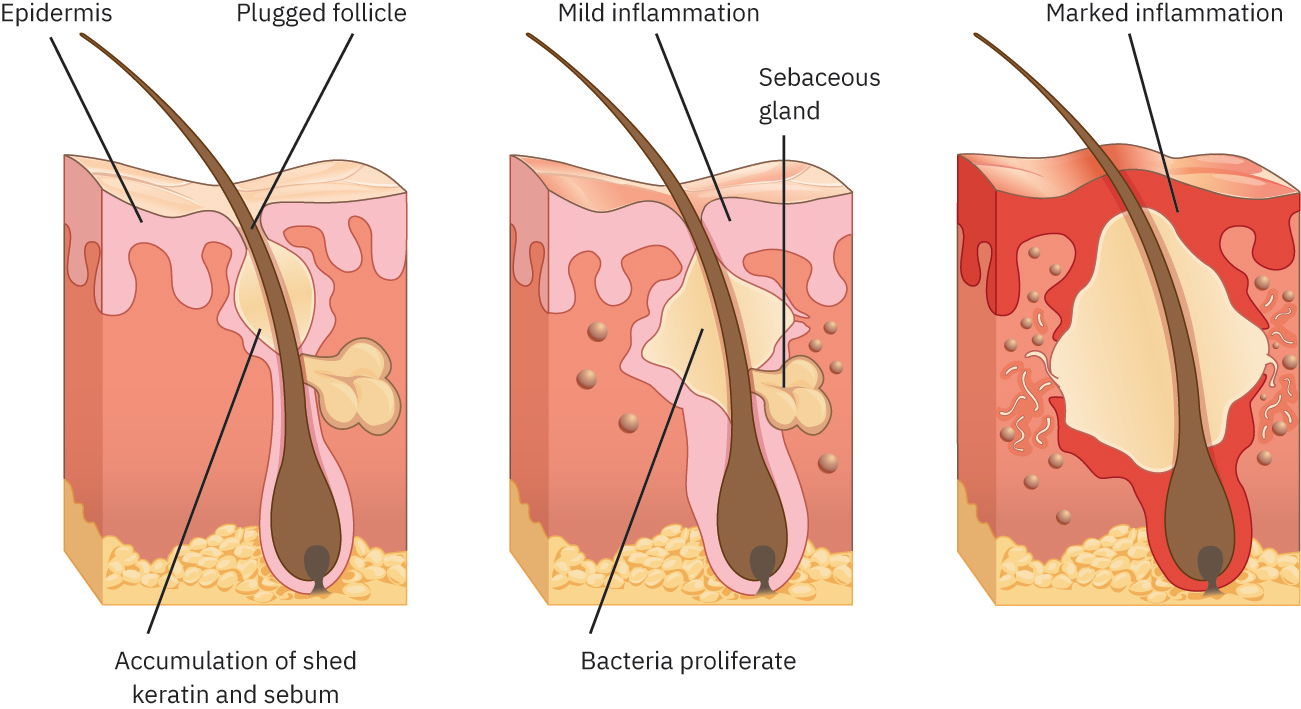 Illustration reference: OpenStax Clinical Nursing Skills Ch.21.2.
Illustration reference: OpenStax Clinical Nursing Skills Ch.21.2.
Hormonal contributors can amplify lesion burden, especially during puberty or endocrine disorders. Oily-skin tendency, family history, medication exposures, and lifestyle triggers can further worsen inflammatory activity and recurrence.
Classification
- Noninflammatory lesions: Open or closed comedones.
- Inflammatory lesions: Erythematous papules and pustules.
- Deep inflammatory lesions: Nodules and cystic lesions with higher scarring risk.
Nursing Assessment
NCLEX Focus
First classify lesion burden and severity, then screen for hormonal contributors, medication risks, and adherence barriers.
- Document distribution (face, neck, chest, upper back), lesion type, tenderness, and progression.
- Screen trigger context including puberty/hormonal shifts, endocrine disorders (for example PCOS), medication exposures, stress, and cosmetic/diet patterns.
- Assess psychosocial impact (self-image distress, social withdrawal, treatment fatigue).
- Confirm whether diagnosis is clinical only or whether endocrine workup is ordered for suspected hormonal contributors.
- In hormonal-evaluation pathways, review ordered labs (for example LH/FSH and androgen-related tests) with provider-plan context.
- Monitor for inflammatory progression and scar-risk features (persistent nodules/cysts, repeated lesion manipulation).
Nursing Interventions
- Reinforce daily gentle skin-care routine and noncomedogenic product selection.
- Administer and teach ordered topical regimens (for example retinoids, benzoyl peroxide, azelaic acid, or topical antibiotics) with adherence coaching.
- Support oral-regimen adherence when prescribed (for example doxycycline, spironolactone, isotretinoin, selected hormonal therapy).
- Teach patients to avoid squeezing or picking lesions to reduce scarring and secondary infection risk.
- Educate on individualized trigger reduction, including diet and product-use modifications when relevant.
- Monitor spironolactone pathways for potassium-surveillance requirements.
- Escalate isotretinoin safety concerns promptly (teratogenicity and serious adverse-effect risk); reinforce close follow-up compliance.
- In adolescent topical-therapy pathways, provide anticipatory side-effect counseling and adherence coaching to reduce early self-discontinuation.
- Reassess treatment response trends and coordinate dermatology referral when symptoms persist or worsen.
Isotretinoin Safety
Isotretinoin requires strict adverse-effect and pregnancy-risk monitoring because severe harm can occur without close follow-up.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| Topical anti-acne agents | Tretinoin, benzoyl peroxide, clindamycin, azelaic acid | Teach consistent application and irritation-management strategy. |
| Oral antibiotics | Doxycycline-class regimens | Use for inflammatory burden when ordered; monitor tolerance and adherence. |
| Hormonal/antiandrogen therapy | Spironolactone, selected oral-contraceptive pathways | Monitor potassium and endocrine-response context; reinforce follow-up labs when ordered. |
| High-risk oral retinoid | Isotretinoin | Requires strict safety monitoring for serious adverse effects and pregnancy risk. |
Clinical Judgment Application
Clinical Scenario
An adolescent presents with painful papules and cystic lesions on the face and upper back, reporting recent worsening and poor confidence at school.
- Recognize Cues: Inflammatory and deep lesion burden with psychosocial impact.
- Analyze Cues: Pattern suggests moderate-to-severe acne with elevated scar risk.
- Prioritize Hypotheses: Impaired skin integrity and adherence-barrier risk are immediate priorities.
- Generate Solutions: Start ordered topical and oral regimen education, trigger review, and safety monitoring plan.
- Take Action: Implement treatment coaching, reinforce no-picking behavior, and schedule reassessment.
- Evaluate Outcomes: Lesion inflammation decreases, new-cyst formation declines, and patient demonstrates sustained self-care adherence.
Related Concepts
- infectious-and-inflammatory-skin-conditions - Broader inflammatory-skin differential and escalation framework.
- polycystic-ovary-syndrome - Hormonal contributor frequently linked with acne burden.
- topical-corticosteroids - Differential/adjunct dermatologic pharmacology context.
- antibiotics - Oral and topical antimicrobial stewardship principles.
- impaired-skin-and-tissue-integrity - Barrier protection and healing-risk framework.
- acne-drugs - Systemic and topical acne-drug framework.
Self-Check
- Which lesion patterns indicate higher long-term scarring risk in acne?
- Why are potassium checks important for patients receiving spironolactone for acne?
- What counseling point is most critical for isotretinoin safety?