Polycystic Ovary Syndrome
Key Points
- PCOS is a common endocrine disorder associated with oligo-ovulation or anovulation and affects an estimated 6 to 12 percent of U.S. reproductive-age persons AFAB.
- Core features include menstrual irregularity, hyperandrogenism, and polycystic-ovary morphology.
- PCOS has reproductive, metabolic, and cardiovascular consequences that extend beyond childbearing years.
- Diagnosis uses Rotterdam criteria after excluding alternative causes.
Pathophysiology
PCOS is a multisystem endocrine condition with heterogeneous presentation. Common biologic patterns include hyperandrogenism and insulin resistance, with possible genetic susceptibility in affected families.
Clinical manifestations vary widely. Some patients first present during infertility evaluation, while others present earlier with irregular cycles, androgenic symptoms, or weight-related metabolic concerns. Frequent symptom clusters include oligomenorrhea/amenorrhea, hirsutism, acne, scalp alopecia, central obesity, and infertility.
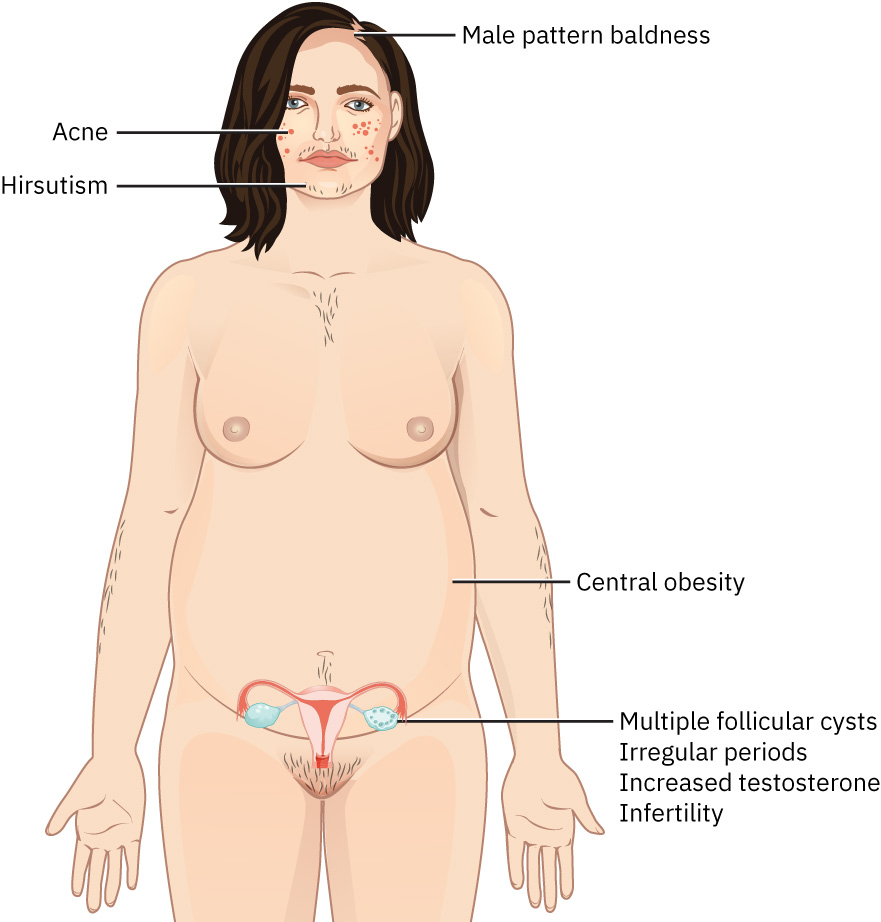 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.6.1.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.6.1.
Unopposed or irregular endometrial exposure from chronic anovulatory patterns can increase endometrial hyperplasia and long-term endometrial-cancer risk if untreated. Metabolic and cardiometabolic burden can include dysglycemia, dyslipidemia, hypertension, and inflammatory-risk amplification. Additional risk domains include obstructive sleep apnea, nonalcoholic fatty liver disease, and mood disorders; these should be included in longitudinal surveillance planning.
Classification
- Ovulatory dysfunction domain: Infrequent or absent ovulation with irregular menstruation.
- Hyperandrogenic domain: Clinical or laboratory androgen excess (for example hirsutism, acne, alopecia).
- Ovarian morphology domain: Polycystic follicular pattern on ultrasound.
- Complication domain: Infertility, cardiometabolic risk, mood burden, and pregnancy-risk amplification.
Nursing Assessment
NCLEX Focus
Use Rotterdam logic (2 of 3 criteria) only after excluding other endocrine/reproductive causes.
- Assess symptom spectrum and onset pattern: cycle irregularity, androgenic changes, weight trends, and fertility concerns.
- Apply Rotterdam criteria context: menstrual irregularity, hyperandrogenism (clinical/lab), and polycystic ovaries on ultrasound.
- Confirm exclusion testing for alternate causes (for example pregnancy, prolactin elevation, thyroid dysfunction, and other hormonal disorders).
- Assess androgen-focused labs when ordered (for example testosterone and DHEAS).
- Assess completeness of initial diagnostic workup (vital signs, pelvic exam, blood testing, and pelvic ultrasound) when diagnosis remains uncertain.
- Screen for metabolic complications after diagnosis: insulin resistance/diabetes, lipid abnormalities, BP elevation, and obesity-linked risk.
- Screen broader comorbidity burden: sleep-disordered breathing, fatty-liver risk, and depression/anxiety symptoms.
- Screen psychosocial burden, including depression/anxiety and body-image distress.
- In pregnancy-capable patients, counsel on higher risk of gestational diabetes, preeclampsia, and preterm birth with PCOS.
Nursing Interventions
- Provide clear education that PCOS is chronic but manageable with combined endocrine, metabolic, and reproductive planning.
- Reinforce lifestyle treatment as foundational care: regular activity, healthy diet, and sustainable weight reduction goals.
- In nutrition counseling, prioritize reduced refined-carbohydrate and added-sugar intake with higher-fiber, whole-food patterns to improve insulin-resistance burden.
- Consider omega-3-rich food inclusion and monitor iron and vitamin D status when intake pattern or symptoms suggest micronutrient risk.
- Teach that even modest weight loss can improve cycle regularity, hormonal profile, and fertility outcomes.
- Support shared decision-making for symptom priorities (cycle regulation, fertility goals, hirsutism/acne, metabolic prevention).
- For metformin use, teach gradual titration with meals, expected GI side effects, and rare lactic-acidosis risk escalation cues.
- Reinforce long-term follow-up for endometrial protection and cardiometabolic risk monitoring.
- Provide nonjudgmental counseling on cosmetic symptom options (depilatories, laser, waxing/shaving, electrolysis, or hair-loss support options).
- Encourage support-group and peer-support engagement when stigma or delayed care-seeking has affected diagnosis and treatment continuity.
Metabolic-Cardiovascular Overlook
Treating PCOS only as a fertility issue can miss high-impact risks such as diabetes, hypertension, dyslipidemia, and cardiovascular disease.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| combined-hormonal-contraceptives | Pill/patch/ring estrogen-progestin pathways | Regulate cycles, reduce endometrial-hyperplasia risk, and improve hyperandrogenic symptoms in selected nonpregnancy-seeking patients. |
| ovulation-induction-agents | Metformin, clomiphene, letrozole contexts | Used for insulin resistance and fertility-focused ovulation support; monitor efficacy by treatment goal and reinforce metformin GI/lactic-acidosis safety teaching. |
| Aldosterone receptor antagonists | Spironolactone contexts | May reduce hirsutism/acne; reinforce monitoring and pregnancy-avoidance counseling when applicable. |
Clinical Judgment Application
Clinical Scenario
A patient reports irregular menses, worsening facial hair and acne, central weight gain, and 14 months of unsuccessful attempts to conceive.
- Recognize Cues: Combined ovulatory, androgenic, and fertility cues are highly consistent with PCOS pattern risk.
- Analyze Cues: Differential requires structured exclusion of pregnancy, thyroid, and prolactin-related causes.
- Prioritize Hypotheses: Priority is confirmatory Rotterdam-based assessment plus metabolic-risk stratification.
- Generate Solutions: Initiate diagnostic workup, lifestyle plan, and goal-based treatment counseling (fertility versus cycle/androgen control).
- Take Action: Coordinate labs/imaging, provide education, and arrange endocrine/gynecologic follow-up.
- Evaluate Outcomes: Diagnosis is clarified, metabolic risks are addressed, and fertility/symptom plan is individualized.
Related Concepts
- functional-reproductive-disorders - PCOS is a core reproductive-endocrine functional disorder.
- causes-of-infertility - PCOS is a leading cause of anovulatory infertility.
- ovulation-induction-agents - Medication pathways for ovulation induction and insulin-resistance support are central in PCOS care.
- ovarian-cysts - PCOS can present with multiple follicular ovarian cystic structures on ultrasound.
- perimenopause-and-menopause - Long-term cardiometabolic risk tracking remains important across later life transitions.
Self-Check
- What are the three Rotterdam criteria, and why must alternate causes be excluded first?
- Which PCOS risks require routine long-term surveillance beyond fertility concerns?
- How can modest weight reduction change reproductive and metabolic outcomes in PCOS?