Transfusion Reactions Types and Nursing Response
Key Points
- Transfusion reactions can be immune or non-immune and range from mild symptoms to life-threatening instability.
- Highest-risk acute reactions commonly emerge within the first 15 to 20 minutes of transfusion.
- Immediate stop-transfusion response with protocol escalation is essential when reaction is suspected.
- Major reaction categories include allergic, anaphylactic, febrile non-hemolytic, acute hemolytic, septic, TACO, and TRALI.
- Early findings can overlap across reaction types, so nurses prioritize immediate safety actions before final subtype confirmation.
- New low-back pain shortly after transfusion start is a high-risk cue for possible acute hemolytic reaction.
Pathophysiology
Transfusion reactions occur when recipient and donor factors interact in a harmful way during or after blood product administration. Immune-mediated mechanisms include antigen-antibody incompatibility and hypersensitivity responses. Non-immune mechanisms include bacterial contamination and volume-related cardiopulmonary stress.
Clinical presentation may overlap across reaction types, so rapid pattern recognition and immediate safety actions are prioritized over delayed differentiation. Early signs such as fever, urticaria, chills, pruritus, dyspnea, and hemodynamic change require immediate reassessment.
Classification
- Allergic (mild to moderate): Pruritus, erythema, urticaria, possible bronchospasm; usually during transfusion to 24 hours after.
- Anaphylactic: Rapid severe hypersensitivity (often IgA-related) with hypotension, respiratory compromise, and possible arrest; commonly within 5 to 15 minutes.
- Febrile non-hemolytic: Cytokine-mediated fever and systemic discomfort, often in immunocompromised recipients; typically an increase of about 1 C from baseline with onset during infusion or shortly after.
- Acute hemolytic: ABO/Rh incompatibility with rapid intravascular hemolysis and systemic instability, often within the first 15 minutes; low-back pain, fullness, hemoglobinuria, hypotension, and tachycardia are high-priority cues.
- Delayed hemolytic: Hemolytic reaction pattern emerging days to weeks after transfusion.
- Septic: Bacterial contamination (commonly platelet-associated storage contamination risk) with high fever and shock risk during transfusion or soon after; rapid chills, vomiting, and marked hypotension are concerning cues.
- TACO: Volume overload pattern with respiratory and circulatory congestion; risk increases with rapid/large-volume infusion.
- TRALI: Non-cardiogenic pulmonary edema after donor-recipient immune interaction, usually during transfusion or within the early post-transfusion window.
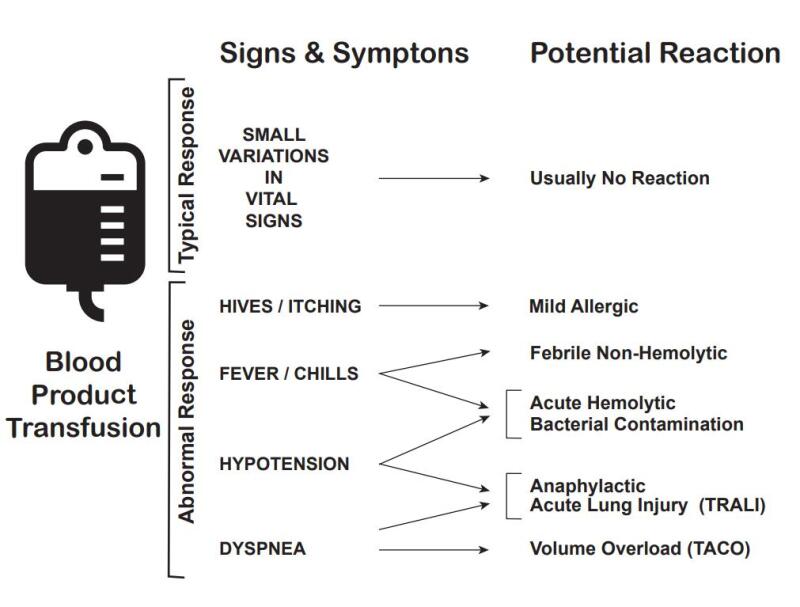 Illustration reference: OpenRN Nursing Advanced Skills Ch.3.2.
Illustration reference: OpenRN Nursing Advanced Skills Ch.3.2.
Nursing Assessment
NCLEX Focus
Prioritize first-15-minute surveillance and immediate differentiation between mild symptoms and evolving cardiopulmonary emergency.
- Obtain baseline physical assessment and vitals before transfusion for later comparison.
- During early infusion, monitor for fever, chills, urticaria, itching, dyspnea, chest/back/flank pain, hypotension, and hemoglobinuria.
- Monitor for neurologic deterioration cues such as anxiety, dizziness, and disorientation with shock progression.
- Monitor for integumentary and volume cues: flushing, hives, chills, and edema pattern suggesting overload.
- Monitor for gastrointestinal and renal cues including nausea, abdominal pain, dark or blood-tinged urine, and worsening hemoglobinuria.
- Watch for volume-overload cues (crackles, JVD, hypertension, tachypnea) suggesting fluid-volume-overload-hypervolemia.
- Watch for severe respiratory failure cues (hypoxemia, cyanosis, non-cardiogenic pulmonary edema) suggesting TRALI pattern.
Nursing Interventions
- Stop transfusion immediately at first suspicion of reaction and notify provider.
- Maintain IV access with new primed 0.9% normal-saline tubing directly attached to vascular access.
- Retain blood product and tubing for laboratory analysis per agency policy.
- Perform frequent vital-sign reassessment (commonly every 15 minutes in acute phase) and implement ordered diagnostics.
- Remain with the patient, compare with baseline status, and maintain slow vein-open saline flow per protocol while escalation is in progress.
- Recheck identifiers, labels, and documentation immediately to identify any clerical mismatch contributing to incompatibility risk.
- Administer ordered treatment based on reaction pattern (for example antihistamine/antipyretic, epinephrine, corticosteroids, diuretic, antimicrobials, oxygen, or ventilatory support).
- For mild reactions, anticipate provider-directed symptom treatment (for example acetaminophen or diphenhydramine) and only resume transfusion if explicitly ordered with close monitoring.
- For TACO risk, follow conservative infusion rates (commonly about 2 to 4 mL/kg/hr) and reassess cardiopulmonary status closely.
- For TACO symptoms, prioritize upright positioning, oxygen support, and diuretic-based volume reduction per orders.
- In known prior allergic or febrile non-hemolytic patterns, anticipate prevention steps such as ordered antihistamine premedication and leukocyte-reduced product selection per policy.
- For suspected acute hemolytic reaction, obtain ordered blood and urine testing and send remaining product/tubing to the blood bank or laboratory immediately.
- For septic-reaction concern, obtain blood cultures and begin ordered broad-spectrum antimicrobial support with hemodynamic monitoring.
- Prepare blood and urine specimen collection promptly and ensure the used blood bag and administration set are sent for transfusion-service evaluation.
Sentinel Safety Threat
Blood incompatibility and delayed response to reaction signs can lead to irreversible harm or death; strict verification and rapid protocol execution are mandatory.
Clinical Judgment Application
Clinical Scenario
Ten minutes after transfusion initiation, a client develops chills, dyspnea, and falling blood pressure.
- Recognize Cues: Early severe reaction signs during high-risk initiation window.
- Analyze Cues: Acute transfusion reaction is likely and may progress rapidly.
- Prioritize Hypotheses: Immediate threat is cardiopulmonary deterioration.
- Generate Solutions: Stop transfusion, switch to new saline tubing, notify provider/blood bank, and prepare emergency medications/support.
- Take Action: Execute reaction protocol and reassess continuously.
- Evaluate Outcomes: Hemodynamics and respiratory status stabilize with no further progression.
Related Concepts
- blood-transfusion-verification-initiation-and-reaction-response - Procedure-level workflow for prevention and immediate response.
- abo-blood-group-compatibility-and-transfusion-safety - Compatibility verification prevents acute hemolytic reactions.
- hypersensitivity-types-and-anaphylaxis-response - Supports rapid management of severe allergic/anaphylactic patterns.
- fluid-volume-overload-hypervolemia - TACO risk recognition and volume-management context.
- acute-respiratory-distress-syndrome - TRALI-like non-cardiogenic pulmonary edema context.
Self-Check
- Which reaction patterns are most likely to present in the first 15 minutes of transfusion?
- Why must new saline tubing be used instead of the existing blood tubing when a reaction is suspected?
- Which clinical findings help differentiate TACO from TRALI at bedside?