Older Adult Dehydration Risk
Key Points
- Older adults have elevated risk for fluid, electrolyte, and acid-base imbalance.
- Common contributors include decreased thirst sensation, disability, cognitive impairment, and medication effects.
- Diuretic use can increase fluid loss and accelerate dehydration progression.
- Dehydration in older adults can present with confusion, falls, and urinary infection risk.
- Acute confusion can reflect hydration decline interacting with renal function and medication metabolism, including UTI-related deterioration.
- Age-related renal changes increase susceptibility to sodium and potassium imbalance (for example hyponatremia and hyperkalemia).
- With aging, thirst-hunger discrimination can decline, so clinically relevant dehydration may already be present when thirst is first perceived.
- Prevention depends on proactive monitoring, routine prompting, and early intervention.
- Some older adults intentionally limit fluids to avoid bathroom trips, which can accelerate dehydration.
Pathophysiology
Aging reduces physiologic reserve and can blunt thirst-driven fluid intake behavior. Combined with chronic disease burden and medication exposure, this increases risk for negative fluid balance and downstream electrolyte or acid-base instability.
Dehydration risk in older adults is multifactorial: low perceived thirst, functional barriers to drinking, cognitive impairment, and therapies that increase fluid loss or impair decision-making. These factors can delay recognition until complications emerge. Age-related renal decline and altered medication excretion can further increase delirium vulnerability when hydration status worsens.
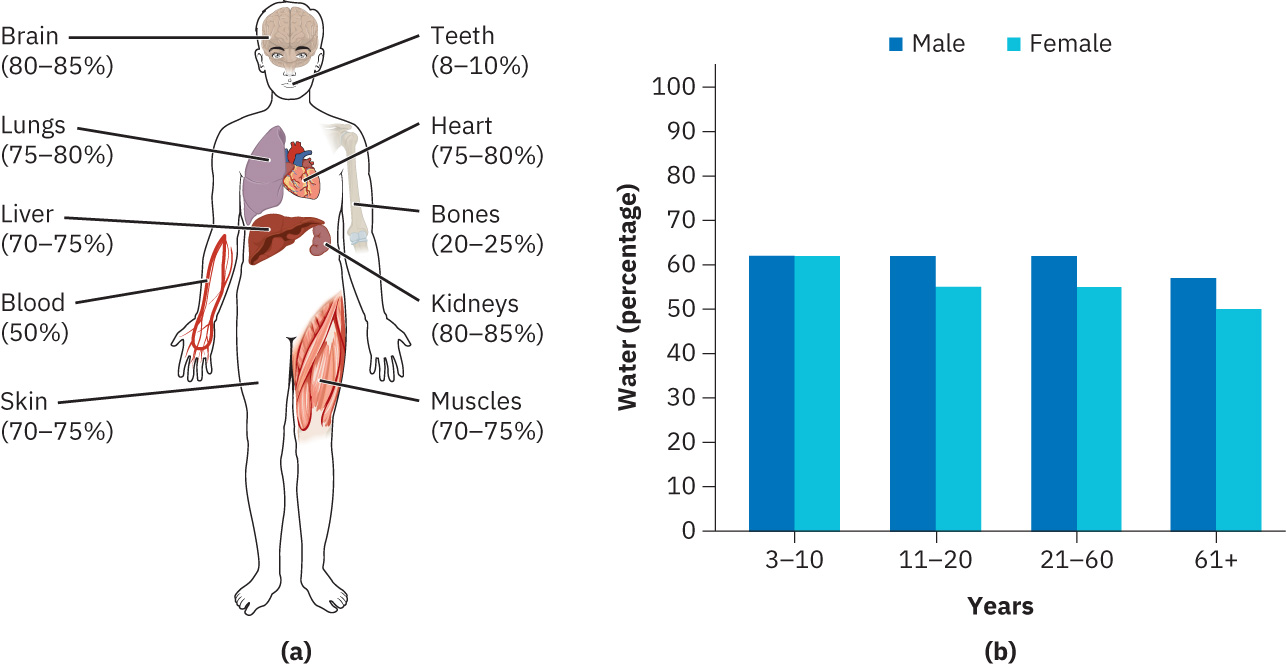 Illustration reference: OpenStax Clinical Nursing Skills Ch.17.1.
Illustration reference: OpenStax Clinical Nursing Skills Ch.17.1.
Classification
- Physiologic risk: Reduced thirst sensation and lower compensatory reserve.
- Functional risk: Disability limits independent hydration behavior.
- Cognitive risk: Dementia or delirium may reduce intake reliability.
- Medication risk: Diuretic-associated volume loss and treatment side effects.
Nursing Assessment
NCLEX Focus
In older adults, monitor hydration trend proactively because symptoms can be subtle and late.
- Track daily intake patterns, weight trend, and intake-and-output balance.
- Assess cognition, mobility, and self-care ability that affect oral fluid intake.
- Assess intentional fluid restriction behaviors related to fear of urgency, incontinence, or nighttime toileting.
- Assess whether hunger cues are being misinterpreted as thirst (or vice versa), because delayed fluid intake can worsen headache, mood, attention, and short-term memory performance.
- Review medication profile for dehydration-promoting effects, especially diuretics.
- Monitor for dehydration cues such as dry mouth/mucous membranes, dry or tented skin, dizziness, headache, tachycardia, hypotension, and darker/scant urine (for example less than about 200-300 mL).
- When checking turgor in older adults, use anterior chest/sternal skin rather than the back of the hand, and interpret cautiously because age-related tissue change can reduce turgor reliability.
- Treat new confusion, gait instability/falls, and urinary-symptom changes as possible dehydration consequences in older adults.
- Treat abrupt confusion or worsening baseline cognitive impairment as possible dehydration/infection signal and evaluate for UTI when clinically indicated.
- Reassess frequently during acute illness or heat exposure periods.
Nursing Interventions
- Implement individualized hydration plans with realistic daily targets.
- Encourage oral fluids routinely even when thirst is not reported.
- Reinforce hydration-first routines (for example offering water before snacks when intake cues are unclear) and individualize daily fluid goals to comorbid conditions.
- Pair scheduled fluid prompts with toileting plans so urinary-frequency concerns do not drive unsafe fluid avoidance.
- Coordinate caregiver support when cognitive or functional barriers are present.
- Reinforce symptom-escalation education and when to seek urgent care.
- Review medication timing and side effects that may worsen fluid loss.
- Use early lab and clinical reassessment when imbalance risk increases.
Silent Deterioration Risk
Older adults may deteriorate without dramatic early symptoms; delayed response increases risk for severe imbalance.
Pharmacology
Medication review is central; diuretics and other agents with dehydration risk should be monitored with hydration trends and symptom surveillance.
Clinical Judgment Application
Clinical Scenario
An older adult on chronic diuretic therapy reports reduced intake and new confusion over two days.
- Recognize Cues: High-risk age group with medication-related fluid-loss factors and neurologic change.
- Analyze Cues: Dehydration with early electrolyte impact is likely.
- Prioritize Hypotheses: Progression risk is high without immediate trend-based intervention.
- Generate Solutions: Intensify monitoring, review medication effects, and reinforce hydration plan.
- Take Action: Escalate concerning changes and implement corrective management.
- Evaluate Outcomes: Intake, cognition, and fluid-balance markers stabilize.
Related Concepts
- prevention-of-fluid-electrolyte-and-acid-base-imbalances - Population-level prevention framework.
- patient-education-for-fluid-electrolyte-and-acid-base-risk - Education strategy for high-risk groups.
- diuretics - Common contributor to dehydration in older adults.
- focused-assessment-for-fluid-electrolyte-and-acid-base-imbalance - Reassessment workflow for worsening cues.
- pediatric-dehydration-risk - Contrasting age-based dehydration risk profile.
Self-Check
- Which age-related factors most often mask early dehydration in older adults?
- Why does diuretic use increase monitoring frequency needs?
- What caregiver supports reduce dehydration risk at home?