Peripheral IV Access
Key Points
- Start with systematic vein assessment in upper extremities and choose the least risky site that meets infusion goals.
- Match catheter gauge and device type to therapy needs, vessel size, and life-span factors.
- Gauge selection is flow-critical: lower gauge number means wider catheter and higher flow potential.
- Prioritize a straight, resilient vein segment on the nondominant upper extremity when feasible, and avoid high-risk sites such as palmar wrist veins.
- Use transparent dressing and securement so site status remains visible and dislodgement risk is reduced.
- Monitor frequently for local and systemic complications and intervene immediately when abnormalities appear.
Equipment
- Peripheral IV catheter (commonly 14-24 gauge range; adults often 18-20 gauge, and frail older adults/pediatric patients often 22-24 gauge)
- Extension tubing or saline lock setup based on whether infusion is continuous or intermittent
- Tourniquet or blood pressure cuff for short vein-dilation use
- Antiseptic supplies, dressing, and securement device (stat lock, chevron tape, arm board/wrap)
Procedure Steps
- Verify the active provider order includes solution/medication type, total volume, infusion rate, duration, and order date/time; complete pre-infusion subjective risk review (medication/latex allergy history, CHF/CKD fluid-overload risk, and current IV-site discomfort during infusion), and perform medication-right checks at preparation/dispensing and again at bedside before administration.
- Assess veins visually and by palpation from hand upward, including common upper-extremity targets (dorsal venous network, median cubital, accessory cephalic, and median antebrachial when appropriate); prioritize distal-first selection to preserve proximal options, and choose a straight, spongy-resilient segment (about 1/4 to 1/2 inch) while avoiding bifurcations, sharp curves, and valve-dense segments.
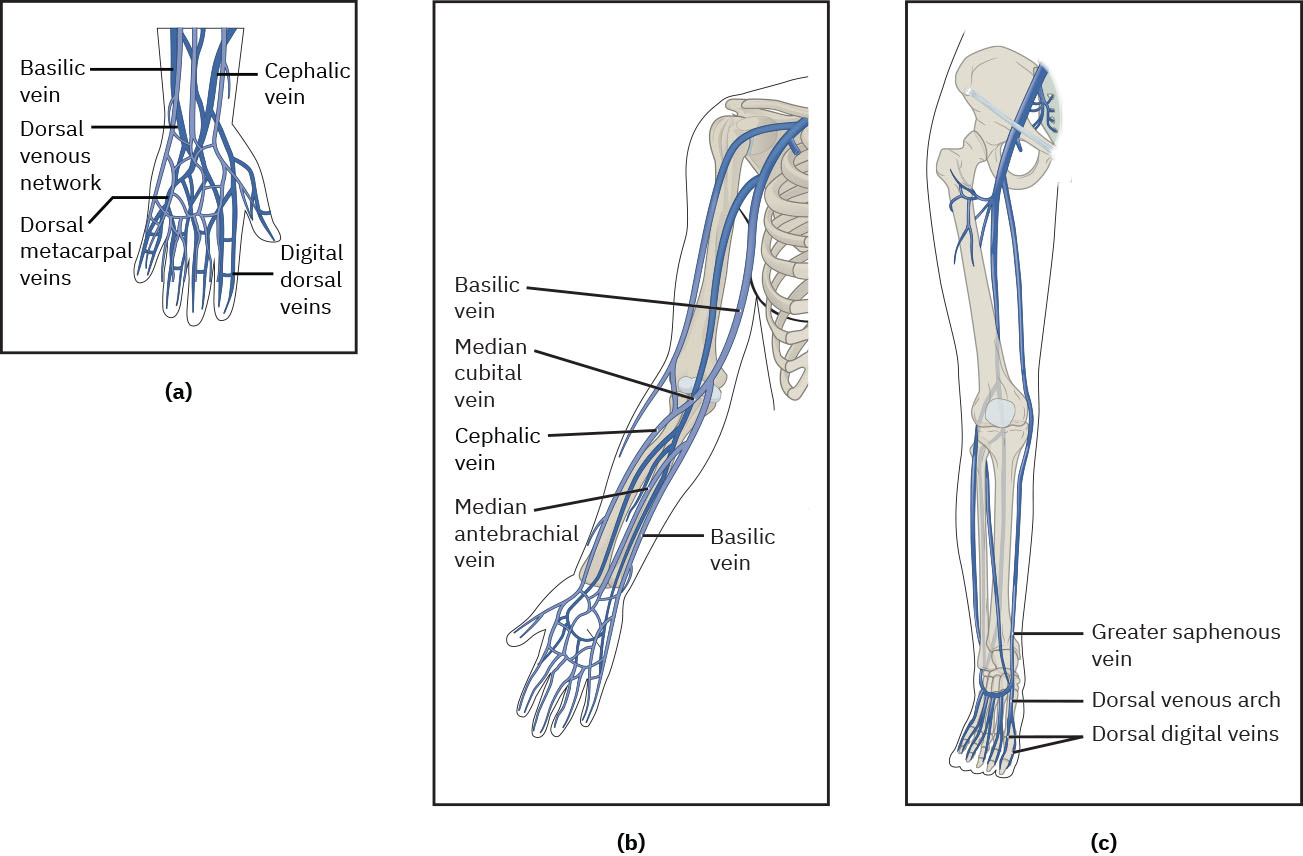 Illustration reference: OpenStax Clinical Nursing Skills Ch.13.
Illustration reference: OpenStax Clinical Nursing Skills Ch.13. - Avoid high-risk sites and limbs with restrictions (palmar wrist veins, mastectomy/lumpectomy or lymph node dissection side, AV fistula arm, lymphedema, DVT, fracture, contracture, extensive scarring, casted/restricted limbs, major sensory deficits such as paralysis/stroke, edema, heavy tattooing that obscures assessment, or limb-alert designation).
- For anticipated multi-day continuous infusions, avoid flexion- or motion-heavy sites (for example antecubital, wrist, and hand) when feasible to reduce occlusion, discomfort, and repeated-site failure.
- If veins are difficult to visualize, use short-duration dilation strategies (tourniquet with distal pulse confirmation, brief BP-cuff inflation, warmth for about 3-5 minutes, dependent arm positioning, and adjunct devices such as vein finders when available).
- Choose catheter size and type based on purpose of access: lower-gauge larger-diameter catheters for rapid fluid or blood products, and smaller-diameter options for fragile or pediatric vessels.
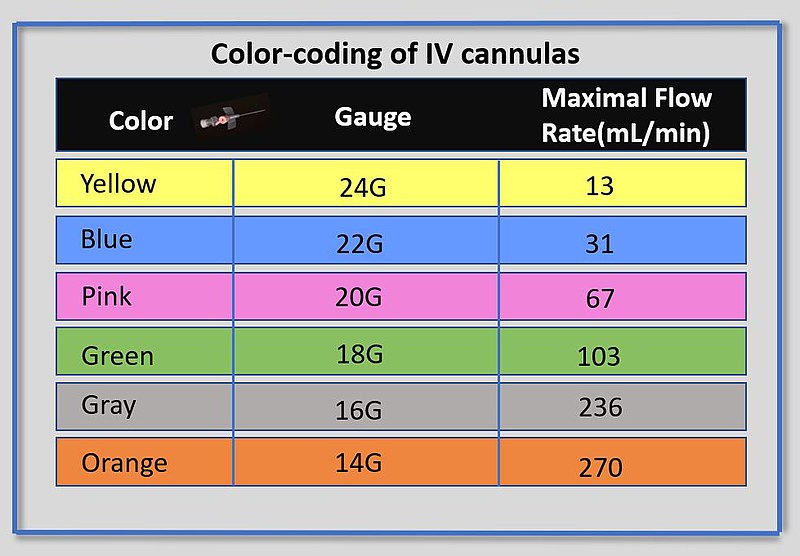 Illustration reference: OpenRN Nursing Advanced Skills Ch.1.3.
Illustration reference: OpenRN Nursing Advanced Skills Ch.1.3. - For vesicant/irritating infusates, prioritize a larger, healthy vein (often more proximal/antecubital if peripheral route is used) and reassess whether central access is safer.
- For very rapid infusion contexts (for example perioperative/critical care), consider larger-bore options such as 16-18 gauge when vessel size and clinical goals support use.
- Verify device compatibility for ordered procedures (for example contrast infusions may require a specific catheter/port profile).
- Prepare and insert using facility aseptic workflow; never override safety-lock needle mechanisms, immediately dispose of sharps after attempt, and reconcile sharps count (brought/opened/disposed) so no needle remains in the environment.
- When preparing primary IV tubing, maintain sterility at spike/ports, preposition clamp, spike the bag, fill drip chamber to about halfway, and fully prime tubing (including inversion/priming of ports when present) until no visible air remains; label bag/tubing date and time per policy.
- Before connecting infusion tubing, reassess site for irritation/infiltration, disinfect the catheter cap with vigorous scrub and dry time (for example initial scrub about 15 seconds), assess patency with 3-5 mL preservative-free saline using a stop-start technique, and do not force flush if resistance occurs.
- Re-disinfect the catheter cap for reaccess (for example at least about 5 seconds per policy), attach tubing aseptically, open clamps, set ordered pump rate or gravity drops/min, reassess site after flow begins, then secure tubing to reduce traction/dislodgement.
- If line is saline locked, flush and clamp per policy when not in use; continue scheduled reassessment and maintenance (site checks, dressing changes, input/output documentation for infused fluids, and escalation for complications).
Ongoing Management
- Perform site surveillance at least every 4 hours in inpatient settings, increase frequency for vesicant infusions, and use higher-frequency checks in high-risk groups (for example every 1-2 hours in critically ill/sedated/cognitively impaired patients and about hourly in neonatal/pediatric settings).
- Reassess IV status at start/end of shift, when pump alarms, before IV medication administration, and whenever the patient reports site pain/tenderness/discomfort.
- Teach outpatient/home patients or caregivers to assess the site every 4 waking hours and report concerns immediately.
- Reassess device appropriateness daily; if IV therapy is expected to continue beyond about six days, evaluate transition to midline or CVAD per policy/provider.
- Use clinically indicated catheter replacement rather than automatic 72-96 hour rotation when no complication is present and policy supports this approach.
- Replace solution bags per policy and generally within about 24 hours of opening/start time; replace immediately if undated, expired, cloudy, or with precipitate, or when a newly prescribed mixture is due.
- Recognize TKO/KVO orders (often 10-20 mL/hr) as line-patency maintenance rates, not full hydration therapy.
- Flush saline locks when not continuously infusing on a routine schedule (commonly every 8-12 hours) using ordered normal-saline volume to maintain patency.
- Typical peripheral saline-lock flush volumes are often about 3-5 mL per policy/order; never force flush against resistance.
- Replace primary/secondary continuous administration sets used for nonblood/nonlipid infusions per policy (commonly every 96 hours, up to 7 days); detached secondary sets are commonly replaced every 24 hours.
- Change peripheral dressings by type (commonly gauze about every 2 days and transparent dressings about every 7 days) and immediately if soiled, loose, wet, bloody, draining, or over compromised skin.
- Replace tubing immediately if contamination or system-integrity compromise is suspected, and label initiation/change date per policy.
- Protect sites during hygiene and daily activity (avoid soaking/tub immersion, cover site for showers, avoid restrictive clothing, and use the opposite arm for blood-pressure cuffs).
Life Span Considerations
- Pediatric and neonatal access planning may require age-specific sites and supports; neonatal access can include hand, foot, or scalp veins (for example frontal/occipital/superficial temporal/posterior auricular) when performed by appropriately trained clinicians.
- Confirm provider guidance before attempting lower-extremity IV access in pediatric patients.
- Improve pediatric success and comfort with securement aids, topical anesthetic options, developmentally appropriate distraction, and clear caregiver role coaching.
- For planned nonemergent pediatric venipuncture/IV starts, use ordered lidocaine-prilocaine topical cream on intact skin with gloves and occlusive coverage; remove before puncture and protect the numb site from heat/cold or injury until sensation returns.
- For children with active infusions, use additional tubing/site protection (for example wrap or arm board when indicated), keep dressings dry, and monitor hourly for patency and fluid-overload cues.
- If joint stabilization is used, apply it so site/pathway remains visible, avoid circulatory constriction or pressure injury, remove periodically for circulation/range-of-motion checks, and avoid wooden tongue depressors in preterm or immunocompromised children because of fungal-infection risk.
- Use age-appropriate explanation before insertion, involve caregiver support when available, and apply comfort measures (for example blanket/toy) to reduce pediatric procedure anxiety.
- In frail older adults (especially with fragile steroid-exposed vessels), consider minimizing tourniquet pressure/use and use a shallower insertion angle for more superficial veins.
- In older adults receiving IV fluids, increase monitoring for fluid-overload signs (for example rising blood pressure/respiratory rate, lower oxygen saturation, edema, crackles, worsening heart-failure pattern) and consider slower rates when venous fragility is present.
Common Errors
- Repeated attempts by the same clinician beyond two insertions → increased pain, delayed therapy, and reduced future access options
- Inadequate securement or infrequent reassessment → higher risk of infiltration, dislodgement, and preventable adverse events
- Continuing use of IV supplies after nonsterile contamination → preventable infection risk; replace catheter or tubing immediately
Related
- infiltration-and-extravasation - Immediate recognition and stop-infusion response are core IV safety actions.
- catheter-related-bloodstream-infection - Strict hand hygiene and aseptic maintenance reduce CR-BSI risk.