Models of Health and Illness in Nursing Practice
Key Points
- Health models shape how nurses assess needs, communicate risk, and design interventions.
- Biomedical models focus on disease processes, while holistic and wellness models include psychosocial and contextual factors.
- Behavior models such as the Health Belief Model and Health Promotion Model guide prevention counseling.
- High-yield behavior-change theories in nursing include Social Cognitive Theory, Theory of Planned Behavior, Health Belief Model, Transtheoretical Model, and Pender’s Health Promotion Model.
- Community-level behavior-change planning can additionally use diffusion of innovations theory to improve adoption of new health practices.
- Need-based models, including Maslow, help prioritize interventions safely.
- Medical-view models extend beyond disease treatment to include spiritual meaning, person-centered growth, and connectedness.
- Health and wellness are related but distinct: health describes multidomain status, while wellness emphasizes active lifestyle choices toward balance.
Pathophysiology
Health models are conceptual frameworks rather than biologic pathways. They organize decision-making by defining what counts as “health,” what drives behavior change, and how risk is interpreted.
Model selection affects care outcomes: narrow disease-only framing can miss social and behavioral drivers, while broad holistic framing may improve long-term adherence and prevention.
Classification
- Biomedical model: Disease-centered diagnosis and treatment emphasis.
- WHO health framing: Health as complete physical, mental, and social well-being, not only absence of disease.
- Holistic/wellness model: Integrated physical, mental, emotional, intellectual, social, spiritual, cultural, and environmental dimensions.
- Holistic Health Model emphasis: Balance across physical, emotional, social, and spiritual domains with prevention focused on root causes (for example nutrition, exercise, stress, and environmental exposures).
- Health-status framing: Interconnected physical, emotional, social, intellectual, and spiritual status domains.
- Wellness-action framing: Active pursuit across physical, emotional, social, occupational, spiritual, intellectual, environmental, and financial dimensions.
- Dunn high-level wellness model: Ongoing growth process using being, belonging, becoming, and befitting domains.
- Behavioral models: Health Belief Model and Health Promotion Model for risk perception and behavior change.
- Cognitive-behavioral common-concepts domain: Behavior is mediated by cognition, knowledge alone is insufficient for change, and perception-motivation-skill-social context jointly shape outcomes.
- Social Cognitive Theory (SCT): Behavior reflects dynamic interaction among personal factors, environment, and prior behavior; self-efficacy strongly predicts planned behavior uptake.
- SCT applied-construct domain: Reciprocal determinism, behavioral capacity, expectations, self-efficacy, observational learning, and reinforcement guide intervention design.
- Theory of Planned Behavior (TPB): Behavior intention is influenced by attitude, subjective norms, and perceived behavioral control; feasibility and access shape follow-through.
- Health Belief Model (HBM) constructs: Perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy.
- HBM strategy-matching domain: Risk personalization, consequence framing, barrier reduction, readiness cues, and confidence-building actions are matched to each construct.
- Transtheoretical Model (TTM): Precontemplation, contemplation, preparation, action, maintenance, and termination with possible nonlinear relapse movement.
- Diffusion-of-innovations domain: Community adoption of new health practices depends on innovation features, communication channels, social-system dynamics, and adoption time course.
- Diffusion-attribute domain: Relative advantage, compatibility, complexity, trialability, and observability influence uptake speed and scale.
- Diffusion-adopter domain: Innovators, early adopters, early majority, late majority, and laggards require tailored engagement strategies.
- Pender Health Promotion Model (HPM) belief set: Perceived benefits, perceived barriers, self-efficacy, activity-related affect, interpersonal influences, situational influences, commitment to action, and immediate competing demands/preferences.
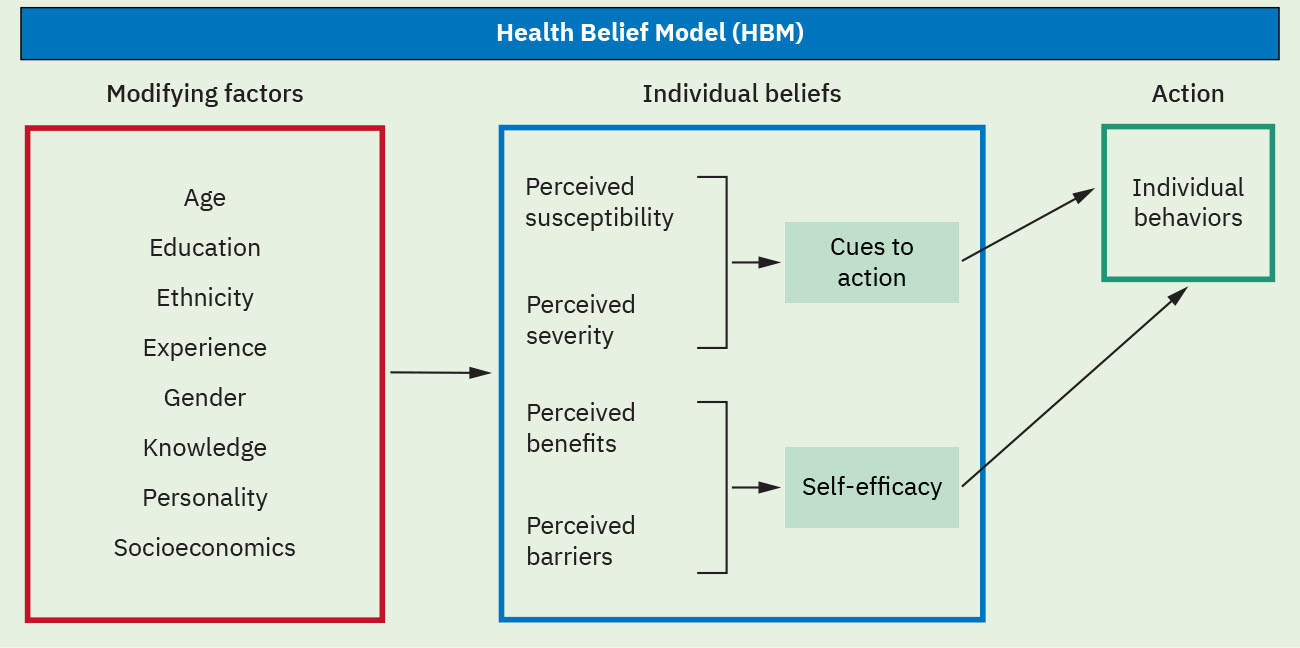 Illustration reference: OpenStax Fundamentals of Nursing Ch.4.2.
Illustration reference: OpenStax Fundamentals of Nursing Ch.4.2.
- Health Promotion Model (HPM) structure: Individual characteristics and experiences, behavior-specific cognitions and affect, and behavioral outcomes.
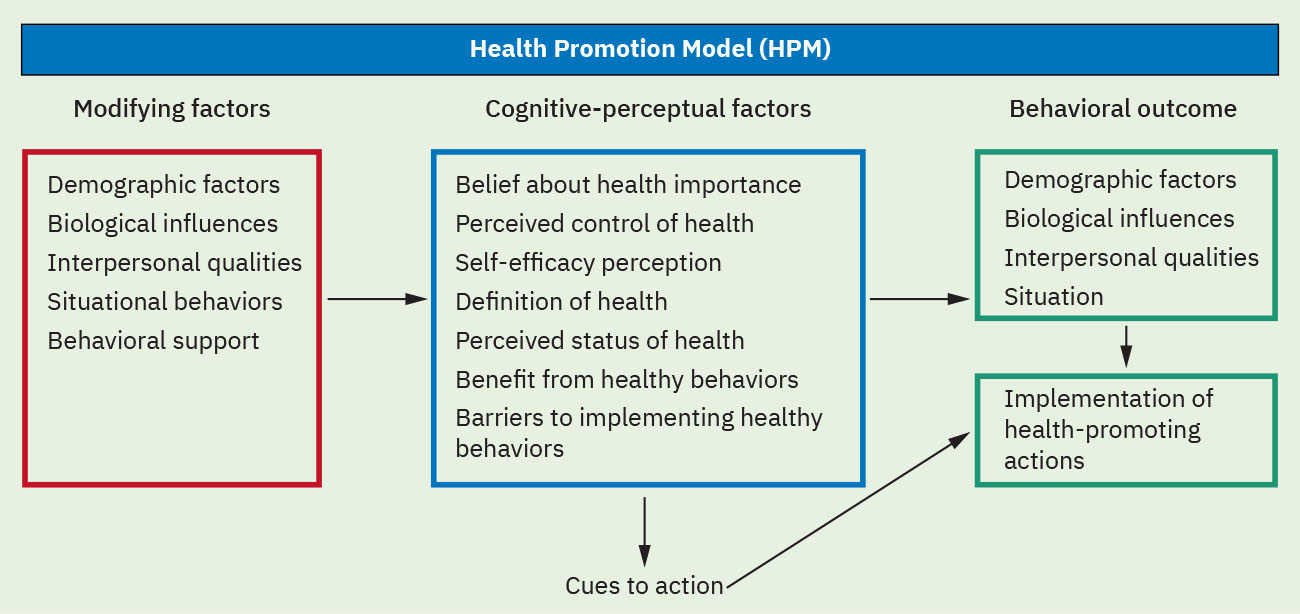 Illustration reference: OpenStax Fundamentals of Nursing Ch.4.2.
Illustration reference: OpenStax Fundamentals of Nursing Ch.4.2.
- Need-priority model: Maslow hierarchy for sequencing care priorities.
- Medical-view models: Religious, humanistic, and transpersonal perspectives on healing and meaning.
- Health-illness continuum models: Biomedical, psychosomatic, and existential frameworks that differ in how body, mind, and purpose are weighted.
Medical-View Model Distinctions
- General medical model: Frames health as absence of disease, emphasizes diagnosis/treatment (for example medication and procedures), and also uses prevention strategies such as vaccines, screening, and lifestyle modification.
- Religious model: Frames health as physical, mental, and spiritual well-being supported by relationship with a higher power, faith practices, and community meaning systems.
- Humanistic model: Prioritizes person-centered care, unique values, self-awareness, personal growth, and collaborative communication based on empathy and mutual respect.
- Transpersonal model: Emphasizes development beyond ego boundaries, spiritual or mystical experience, and interconnectedness with a larger whole.
Health-Illness Model Contrasts
- Biomedical: Body-as-system framing; strongest for acute disease mechanisms but may underweight psychosocial context.
- Psychosomatic: Psychological distress can manifest as physical symptoms, reinforcing mind-body interaction.
- Existential: Focuses on meaning, authenticity, responsibility, and how individuals respond to uncertainty, suffering, and mortality.
Nursing Assessment
NCLEX Focus
Match model choice to the clinical problem: acute physiologic instability versus long-term behavior change.
- Assess whether current plan overemphasizes disease treatment and underaddresses behavior/context.
- Assess whether the patient equates health only with physical symptoms while neglecting emotional, social, or lifestyle domains.
- Assess patient beliefs about susceptibility, severity, benefits, and barriers.
- Assess intention drivers and TPB elements (attitude, subjective norms, and perceived behavioral control).
- Assess readiness for health-promoting behavior change.
- Assess stage of change (including relapse movement) before choosing intervention intensity.
- Assess unmet basic needs that block higher-level engagement.
- Assess model fit across acute, chronic, and preventive care contexts.
- Assess whether distress patterns suggest psychosomatic contributors or existential meaning conflict.
- Assess spiritual beliefs and community support when patients use religious or transpersonal healing frames.
Nursing Interventions
- Use biomedical framing for urgent physiologic stabilization needs.
- Integrate holistic assessment into chronic and recovery planning.
- Address root causes of imbalance and coach informed daily choices that support whole-person well-being.
- Use Dunn-aligned coaching: strengthen self-awareness (being), connectedness (belonging), growth goals (becoming), and preventive self-care choices (befitting).
- Apply belief- and motivation-based counseling for prevention goals.
- Use SCT-informed coaching to build self-efficacy through small wins, modeling, and supportive feedback.
- Use TPB-informed counseling to target attitude, norms, and practical control barriers in parallel.
- Use staged, realistic health-promotion goals tailored to readiness.
- Use HBM constructs to identify whether low perceived threat, high barriers, or weak cues to action are limiting uptake.
- Use HPM belief mapping to individualize nursing counseling and reduce immediate competing-demand failure.
- Use SCT construct-matched coaching: skills training, small-step goals, modeling, and reinforcement to improve sustained behavior change.
- Use diffusion-of-innovations planning for community programs by simplifying complexity, improving trialability, and targeting early adopters to accelerate spread.
- Build plans that improve patient empowerment and access to supportive environments.
- Pair prevention counseling with ongoing education and skill-building for sustained behavior change.
- Integrate patient values when goals include spiritual practices, nontraditional therapies, or meaning-centered care preferences.
- Reassess and shift model emphasis as patient context changes.
Model Rigidity Risk
Applying one model rigidly to all situations can produce incomplete plans and weaker outcomes.
Pharmacology
Medication plans improve when biomedical prescribing is combined with behavior-focused adherence support and contextual barrier assessment.
Clinical Judgment Application
Clinical Scenario
A patient with hypertension repeatedly misses follow-up and declines lifestyle changes despite understanding diagnosis details.
- Recognize Cues: Biomedical understanding exists, but behavior change is limited.
- Analyze Cues: Belief, motivation, or barrier factors are likely unaddressed.
- Prioritize Hypotheses: Health-belief and promotion models are needed in addition to disease model.
- Generate Solutions: Elicit perceived barriers, set small goals, and align supports.
- Take Action: Implement mixed-model care plan with follow-up coaching.
- Evaluate Outcomes: Adherence and risk-factor control improve.
Related Concepts
- maslows-hierarchy-of-needs - Need-priority framework for safe sequencing.
- humanistic-theories-and-therapies - Person-centered growth, empathy, and self-awareness framing.
- healthy-people-2030-health-equity-and-social-determinants - Population-level prevention orientation.
- evidence-based-decision-making-in-nursing - Model-informed decision integration with evidence.
Self-Check
- When is a biomedical model necessary but insufficient?
- How do Health Belief and Health Promotion models differ in practical use?
- Why should model selection evolve over the course of care?